Ulcerative Colitis (UC): Classification, Symptoms, Diagnosis, and Treatment
Aleksandr F.Abdominal surgeon, MD
30 min read·January 29, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Ulcerative colitis (UC), one of the two types of inflammatory bowel disease (IBD), is a chronic polyfactorial disease with an autoimmune component characterized by the formation of ulcerative and destructive changes in the wall of the colon.
Relevance and epidemiology
A global increase in the incidence of UC is observed worldwide. The highest incidence in the Americas is reported for Canada (16.7 per 100,000 population). In Europe, the incidence of UC ranges from 1.6 to 11.9 per 100,000 population, with more patients observed in Northern European countries. In the East, UC is less common, with the highest incidence observed in Korea (3.62 per 100,000).
Although ulcerative colitis can occur at any age, the peak incidence is noted in the second to fourth decades of life, with a second peak in the sixth decade. Men and women suffer with the same frequency.
Anatomy
The mucosa of the colon is lined with a single-layer columnar epithelium forming a villous layer, essential for maintaining intestinal homeostasis and functioning as a physical and biochemical barrier, serving as a coordinating center for immune protection and cross-interactions between bacteria and immune cells.
This layer consists of invaginations known as “crypts of Lieberkühn.” Intestinal stem cells responsible for the rapid renewal of intestinal epithelium are located at the base of these crypts and develop into transient proliferative cells that differentiate while passing through the transition zone, where intestinal epithelial cells eventually enter the intestinal lumen at the crypt tops.
Intestinal epithelial stem cells can specialize into many cell types, including:
Enterocytes;
Paneth cells;
Goblet cells;
Neuroendocrine cells.
Most cells present in the colon are absorptive by nature (involved in the absorption of electrolytes and fat-soluble molecules), except for crypt cells (which are goblet and enteroendocrine cells) that are secretory.
Goblet cells comprise about 10% of all intestinal epithelial cells. They play an essential role in immunity by synthesizing and secreting mucin (a viscous fluid enriched with glycoproteins), lubricating the intestinal wall, facilitating the movement of chyme, and enabling effective diffusion of intestinal contents.
Goblet cells also act as a physical barrier, protecting the intestinal wall from digestive enzymes and bacterial adhesion to the underlying epithelium. Additionally, these cells produce and secrete biologically active substances that contribute to innate immunity: tripeptides, resistin-like molecule β (RELMβ), and Fc-γ-binding protein (Fcgbp), which inhibit intestinal nematode chemotaxis and stabilize the mucosal layer.
Enteroendocrine cells, producing and secreting hormones, comprise 1% of the colon’s epithelium. One of these molecules is vasoactive intestinal peptide (VIP), a peptide hormone that inhibits the release of gastrin and acid secretion and stimulates water and electrolyte secretion by the small and large intestine.
Since VIP plays an important role in regulating intestinal mucosal integrity and epithelial barrier homeostasis, changes in VIP concentrations in tissues are associated with an increased propensity for inflammatory bowel disorders (colitis).
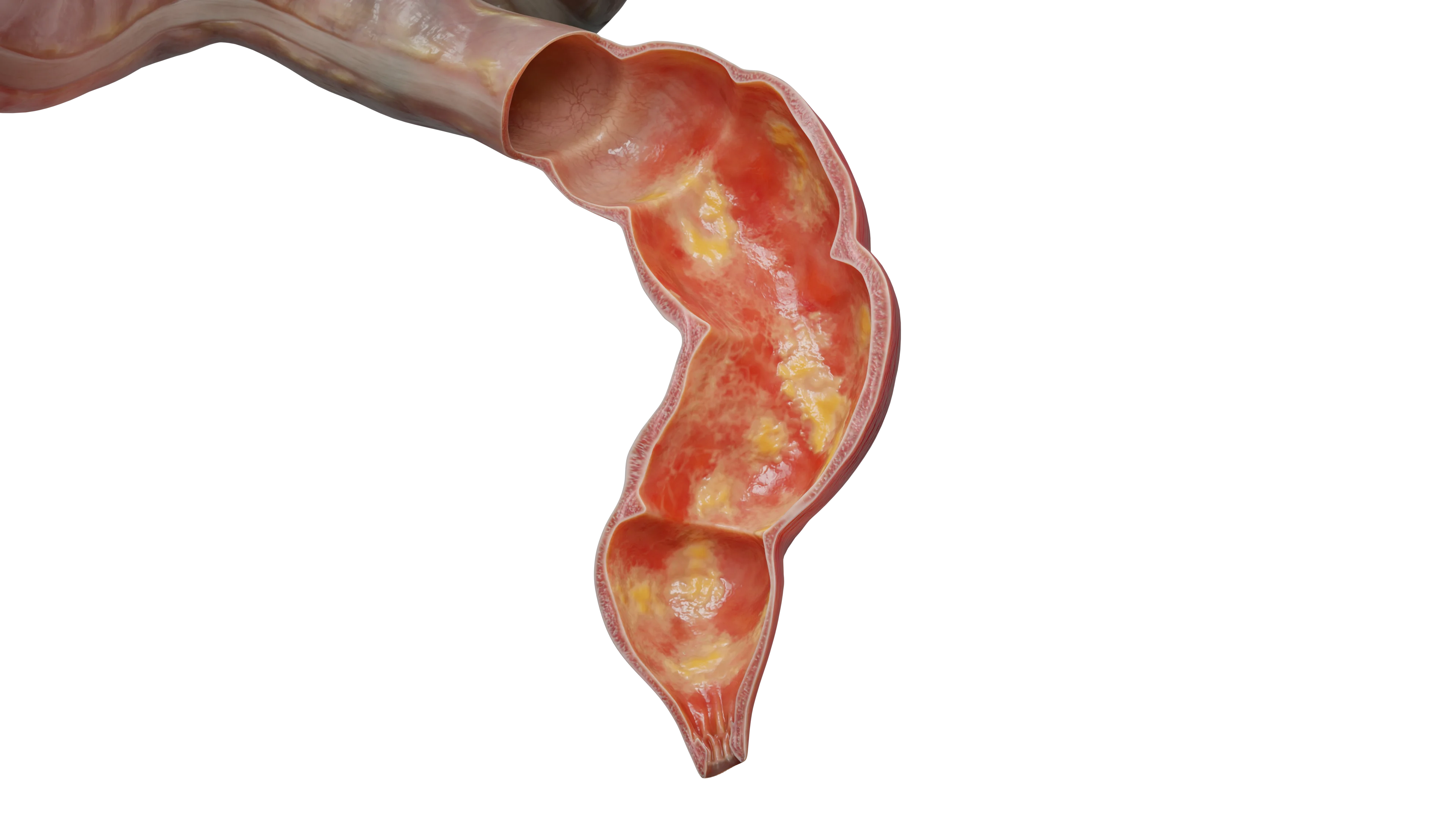
Structure of the colon wall (see text above): 3D model
Etiology and pathogenesis
Ulcerative Colitis is a complex disease resulting from the intricate interaction of genetic susceptibility and environmental triggers, leading to the disruption of the immune system’s response, resulting in chronic inflammation of the colon.
UC is a multifactorial disorder including:
Genetic predisposition.
Epithelial barrier defects.
Dysregulation of immune responses.
Environmental factors.
Proper functioning of specialized intestinal epithelial cells is crucial for maintaining intestinal homeostasis, and their dysfunction play a central role in the pathogenesis of UC. A common histological feature identified in UC is architectural distortion of intestinal epithelium characterized by shortening and reduced branching of crypts. This microscopic change in chronic UC can be observed in every biopsy fragment from the affected colon.
The lamina propria of the colon also contains immune cells, including macrophages, dendritic cells, plasma cells, and lamina propria lymphocytes. These immune cells, along with the genetic predisposition of UC patients, play a crucial role in the progression of UC. A recent genome-wide association meta-analysis identified 163 chromosome loci associated with inflammatory bowel diseases. These loci contain genes involved in autophagy, microbial recognition, lymphocyte signaling, endoplasmic reticulum stress response, and cytokine signaling.
In addition to the genetic profile of UC patients, it is important to note that the disease itself includes pathological immune reactions against intramural and mucosal antigens, which typically involve saprophytic bacteria. Chronic inflammatory reaction is believed to occur following infection with a pathogenic microorganism (e.g., Shigella spp. or Campylobacter spp.), which remain in intestinal tissues.
Exposure to microbial peptides that share immunogenic elements with self-antigens results in the disruption of immune response to the intestine’s own wall antigens. Therefore, a possible basis for UC is a destructive inflammatory response aimed at self-antigens, which are part of the mucin content, goblet cells, and colonocytes.
Local production of these autoantibodies is stimulated by T-cell abnormalities located in the epithelial cell layer and lamina propria of the colon. Autoantibodies detected in the serum of UC patients include antibodies to the colon and antineutrophil cytoplasmic antibodies (ANCA). They are involved in antibody-dependent cell-mediated cytotoxicity, which is presumed to cause damage to the colonic mucosa.
Risk factors
Genetic predisposition: despite only 8–14% of patients with ulcerative colitis having a family history of inflammatory bowel disease (IBD), first-degree relatives of patients diagnosed with UC have a fourfold higher risk of developing similar pathology.
Diet: although there is no specific diet that may aid in the treatment of UC, some studies suggest a connection between higher consumption of certain foods and a potentially increased risk of being diagnosed with UC.
Microbiome: the human gut microbiota is the largest microbial community in the body, containing over 35,000 species of bacteria. Based on DNA sequencing, an accurate characteristic of the gut microbiome in UC patients was obtained, which significantly differs from the microbiome composition of healthy individuals.
Smoking: compared to non-smokers, the incidence of UC in smokers is lower. However, abrupt cessation of smoking is associated with a significant increase in the incidence and severity of the course of UC. Nevertheless, health care professionals believe the risks of smoking far outweigh any potential benefits related to colitis and strongly advise against smoking for everyone, regardless of the presence or absence of IBD.
Appendectomy: similar to the associations noted regarding smoking, appendectomy potentially exerts a protective effect in preventing UC. In a study of more than 200,000 patients who underwent an appendectomy, the incidence of ulcerative colitis was significantly lower than among patients without such a history.
Living conditions and hygiene: the influence of hygiene and living conditions on the risk of developing IBD has long been discussed. One of the hypotheses is that these exposures in early childhood stimulate the diversity of microbiota and the maturation of intestinal immunity. A general review of meta-analyses showed that living near farm animals, having a personal bathroom, having access to hot water, and having pets reduce the risk of developing ulcerative colitis.
Medications: the use of antibiotics is believed to alter the gut microbiome, which may play a role in the pathogenesis of ulcerative colitis. The microbiome is most unstable during childhood, and disturbances in microbiota in the early years of life can alter intestinal immunity and hence susceptibility to IBD.
Stress.
Classification of Ulcerative Colitis
By localization
Ulcerative proctitis: inflammation is limited to the area closest to the anus (rectum).
Left-sided colitis: the inflammation extends from the rectum upwards, involving the sigmoid and descending colon.
Left-sided ulcerative colitis (the rectum, sigmoid, and descending colon are involved): 3D model
Extensive ulcerative colitis: inflammation affects a large part of the colon, but not the entire colon.
Subtotal colitis (the left flank and transverse colon are affected): 3D model
Pancolitis: total involvement of the entire colon.
Total colon involvement in ulcerative colitis: 3D model
By severity (Montreal classification)
Stage
Description
S0 (Remission)
Complete absence of symptoms
S1 (Mild)
Stools up to 4 times/day; blood may be present. Pulse, hemoglobin, temperature, and ESR are normal
S2 (Moderate)
Stools >4 times/day with blood. Minor pulse and temperature deviations
S3 (Severe)
Stools >6 times/day with blood. Pulse >90, temperature >37.5 C, anemia (Hb 105), ESR >30
By the nature of the course
Acute: up to 6 months from the onset of disease.
Chronic progressive: absence of clear episodes of remission during the course of the disease despite treatment.
Chronic relapsing: a course with episodes of remission lasting more than 6 months.
Clinical presentation
Symptoms of ulcerative colitis may vary depending on the severity of the inflammation and its location. The course of ulcerative colitis is characterized by alternating periods of exacerbation and remission.
Most characteristic symptoms:
Diarrhea (often with blood or pus).
Rectal bleeding: discharge of a small amount of blood with stool.
Abdominal pain and cramps.
Rectal pain.
Urgent (intolerable) urge to defecate.
Inability to defecate despite urgent urges.
Weight loss.
Increased fatigue (which may be caused by the disease itself, anemia, or lack of sleep if constantly getting up at night due to pain or diarrhea).
Fever.
In children – growth retardation.
Features of the clinical presentation by localization
The features of the clinical presentation can also be divided depending on the localization of the process.
Proctitis: only the rectum is affected by the inflammation. This means that the rest of the colon is unaffected and can function normally. The main symptom in this variant is the discharge of fresh blood or mucus mixed with blood during defecation. Diarrhea or constipation may occur, as well as frequent false urges to defecate (tenesmus).
Proctosigmoiditis: symptoms are similar to those of proctitis, although constipation is less common.
Left-sided (or distal) colitis: inflammation affects the distal part of the colon; symptoms include diarrhea with blood and mucus, pain in the left side of the abdomen, imperative urges, and tenesmus.
Extensive and total colitis: it may cause very frequent diarrhea with blood, mucus, and sometimes pus. Severe cramps and abdominal pain, tenesmus, fever, and weight loss may occur.
In the setting of the disease, extraintestinal symptoms often develop: joint tenderness and swelling (similar to arthritis), mouth ulcers, swelling and infiltration of the subcutaneous adipose tissue by a type of erythema nodosum, eye irritation and redness (conjunctivitis), onset or exacerbation of osteoporosis.
Extraintestinal manifestations
Joints: arthritis (swelling and pain) appears in about 1 in 10 people with colitis. Most commonly affected are elbows, wrists, knees, and ankles, but joints of the spine and pelvis can be affected as well. Joint problems may appear and disappear during exacerbation but sometimes occur isolated (even without any bowel symptoms).
Liver: primary sclerosing cholangitis (PSC) occurs in 1 in 25 people with colitis. PSC causes inflammation of the bile ducts and may ultimately affect liver cells. Symptoms include fatigue, pain, itching, jaundice, and weight loss.
Skin: erythema nodosum occurs in about 1 in 10 people with colitis. It causes painful red swellings, usually on the legs, which then disappear, leaving a bruise. This condition occurs during flare-ups and is usually controlled when colitis is treated. Less commonly, gangrenous pyoderma may develop in people with colitis. It begins with small, painful blisters that turn into painful, deep ulcers. They can occur anywhere on the skin but are most often found on the shins or around the mouth. This condition is most often associated with flare-ups (though it may occur outside such episodes).
Eyes: the most common disease is episcleritis, which affects the layer covering the white of the eye, causing redness, pain, and inflammation. Episcleritis tends to flare up along with colitis and may require anti-inflammatory treatment; sometimes steroid drops are prescribed. Uveitis (inflammation of the iris) and scleritis (affecting the sclera) may also be associated with colitis. These are serious conditions that can lead to vision loss if not adequately treated. Treatment includes steroid drops, and sometimes immunosuppressants or biological agents are required.
Bones: people with colitis are at greater risk of developing osteoporosis. This may be associated with the inflammatory process itself, poor absorption of calcium needed for bone formation, and low levels of calcium due to avoiding dairy or taking steroids. For prevention and treatment, weight-bearing exercise, calcium intake, vitamin D supplementation, and specific drug therapy are indicated.
Mouth: mouth ulcers or sores occur in about 1 in 25 people with colitis, typically during flare-ups. These ulcers may be minor and disappear within several weeks, but sometimes persist for many weeks and may require steroid treatment.
Hair: hair loss is observed in about one-third of people with Crohn’s disease or ulcerative colitis, more than usual. This type of hair loss is called telogen effluvium (hair shedding). Telogen effluvium can be caused by many factors, including significant exacerbations, poor nutrition, iron and zinc deficiencies, certain medications, and surgical interventions. Hair loss often occurs several months after a trigger, making it difficult to pinpoint the underlying cause. Most people experience full hair regrowth when remission is achieved.
Heart and circulation: people with Crohn’s disease or colitis are about twice as likely to develop blood clots in veins, including deep vein thrombosis (DVT) of the legs. To prevent and reduce risk, smoking cessation, maintaining maximum mobility, consuming large amounts of fluids, and wearing compression stockings are recommended. People with active colitis may also have a slightly increased risk of cardiovascular disease, including heart attacks and strokes.
Complications
Severe bleeding and anemia.
Severe dehydration.
Osteoporosis (loss of bone mass).
Inflammation of the skin, joints, and eyes.
Increased risk of clotting in veins and arteries.
Strictures: narrowing of the intestines due to prolonged inflammation, which can impede the passage of chyme through the colon.
Perforations: very active inflammation of the intestinal wall or severe obstruction caused by a stricture can sometimes lead to perforation (rupture) of the intestine. Through this defect, intestinal contents can leak into the abdominal cavity, leading to peritonitis.
Toxic megacolon: extensive and severe inflammation can cause gases to accumulate in the colon, resulting in its distension. This complication can occur in one out of 40 people with colitis. Symptoms include high fever, abdominal pain, abdominal bloating, and absence of stool. If not treated in a timely manner, this complication may require surgical intervention.
Fistulas: an abnormal passage connecting one internal organ to another or to the body’s external surface. Most fistulas originate in the intestinal wall and connect parts of the intestine to each other, the vagina, bladder, or skin (especially around the anus). Fistulas very rarely occur in people with colitis and are more commonly seen in people with Crohn’s disease.
Increased risk of colon cancer. Ulcerative colitis is not a form of cancer. However, the risk of developing colon or rectal cancer increases with the chronic long-term course of the disease. This risk increases with the extent of colonic involvement by colitis, being higher in extensive colitis than in left-sided colitis. In people with proctitis, this risk is minimal. Research shows that the risk of cancer development usually starts to increase approximately 8-10 years after the onset of IBD symptoms. This does not occur from the date of diagnosis, which may be much later, but from the beginning of the initial symptoms of UC. This means that in the presence of total, extensive, or left-sided ulcerative colitis for eight years or longer, more frequent surveillance colonoscopies should be performed to detect signs of dysplasia or cancer.
Growth failure and developmental delay in children (due to malabsorption of nutrients and losses of significant nutrients).
Diagnosis
History: includes a family history of inflammatory bowel disease, typically in the age group of 20-40 years.
Complaints: periodic diarrhea with bleeding and abdominal pain.
General clinical tests: anemia in CBC, leukocytosis might occur during exacerbations, positive fecal occult blood test.
Endoscopy: colonoscopy or sigmoidoscopy. Biopsies are often taken during endoscopy.
Radiographic methods: MRI and CT of the abdominal organs.
Ultrasound of the abdominal organs: (although it is sometimes difficult to distinguish ulcerative colitis from other inflammatory bowel diseases).
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of ulcerative colitis
Medical therapy
Pharmacological treatment of colitis is aimed at symptom reduction and exacerbation control, followed by remission maintenance once the condition is controlled. Mild and moderate exacerbations can typically be treated at home. However, more severe exacerbations require inpatient treatment.
The main groups of drugs are:
Aminosalicylates (5-ASAs): reduce inflammation in the intestinal mucosa. Examples include mesalazine (Asacol, Ipocol, Octasa, Pentasa, and Salofalk), olsalazine (Dipentum), sulfasalazine (Salazopyrin), and balsalazide (Colazide).
Corticosteroids (steroids): act by blocking substances that trigger allergic and inflammatory reactions in the body. These include prednisolone, prednisone, methylprednisolone, budesonide (Cortiment), hydrocortisone, and beclometasone dipropionate (Clipper).
Immunosuppressants: suppress the immune system and reduce the inflammation level. Main immunosuppressants used for IBD include azathioprine (Imuran), mercaptopurine or 6MP (Purinethol), methotrexate, cyclosporine, and tacrolimus. These are often used for patients who relapse after stopping steroids.
Biological agents: the newest group of medications used for treating IBD. Anti-TNF agents, such as infliximab (Remicade, Remsima, Inflectra), adalimumab (Humira), and golimumab (Simponi), target a protein in the body called TNF (tumor necrosis factor), preventing inflammation. Another type of biological agent is vedolizumab (Entyvio), which prevents WBCs from entering the intestinal mucosa and developing inflammation.
Other medications may be used for alleviating symptoms of ulcerative colitis rather than reducing inflammation.
Symptomatic therapy:
Pain relievers (Paracetamol): it is best to avoid NSAIDs (non-steroidal anti-inflammatory drugs), such as ibuprofen and aspirin, as they can worsen IBD or trigger exacerbations.
Antidiarrheal medications: loperamide (Imodium, Arret) and diphenoxylate (Lomotil). They work by slowing the contractions (muscle movements) of the intestine, so food moves more slowly. It is crucial not to use them during an exacerbation, as this can lead to serious complications.
Laxatives: Movicol (Macrogol, Fortrans). They help relieve constipation by increasing the amount of water in the colon, making stools softer and easier to pass.
Bulking agents (Fybogel): made from plant fibers and facilitate bowel movements.
Antispasmodics: hyoscine butylbromide (Buscopan) and mebeverine can reduce painful cramps and spasms by relaxing muscles. They are most often recommended for patients with IBS but can sometimes be helpful for patients with IBD.
Vitamin and mineral supplements: more common in children to support growth, as well as in adults with significant absorption issues.
Surgical therapy
If conservative therapy is ineffective or significantly impacts quality of life, or in the case of severe UC complications, surgical treatment may be performed: a surgery to remove part of the affected colon or the entire colon (colectomy).
Approximately 1 in 4 patients with ulcerative colitis may ultimately require surgery, depending on the severity of the disease and the affected sections of the colon. Patients with extensive or total colitis are more likely to require surgery than those with proctitis. Surgery may be recommended if cancer or dysplasia (precancerous changes) is detected in the colon.
Types of surgeries:
Subtotal colectomy: the most common type of surgery for colitis. The colon is removed, but the rectum is left with an ileostomy created. Subsequently, a second surgery is performed to close the fistula and restore passage (as inflammation subsides, usually after 2-3 months).
Primary colectomy with the formation of an ileoanal anastomosis: the entire colon and rectum are removed, leaving the anus; a reservoir is formed from the lower end of the ileum, which is connected to the anus, and a temporary looped preventive ileostomy is created (this allows the anastomosis with the anus to be unloaded until the reservoir heals). Following this, an operation is conducted to close the fistula and restore passage.
Colectomy with permanent ileostomy: the colon, rectum, and anal canal are removed, forming a permanent ileostomy.
Colectomy with ileorectal anastomosis: the colon is removed, and the end of the ileum is connected to the rectum without stoma formation. However, this operation is only possible with mild or absent rectal inflammation and a low long-term cancer risk.
Dietary modification
Extensive research has been conducted on the role of diet in ulcerative colitis, but there is still little evidence to suggest that any specific food or supplement can cause or ease colitis progression. Generally, it is essential to maintain a nutritious and balanced diet to support protein and energy balance, as well as drink adequate amounts of fluids to prevent dehydration.
Nonetheless, certain food items affect the symptoms of the disease.
During exacerbation: plain, soft food is recommended during a flare-up of UC, as it causes less discomfort than raw vegetables or spicy food. Consuming too much fiber can increase the urge to defecate. The urge to defecate is usually caused by inflammation in the lower parts of the colon, but as fiber increases stool volume, it may act as a trigger and intensify the urge. Therefore, it might be beneficial to reduce fiber intake and switch to a low-fiber diet during flare-ups.
In remission: after the flare-up subsides, you should attempt to increase your fiber intake again. Fiber is beneficial, as it supports colon health and serves as an energy source for beneficial bacteria.
Triggers: some individuals with colitis notice that dairy products trigger their symptoms, although research has not demonstrated any such pattern.
Alternative treatments
Some patients with ulcerative colitis report that complementary and alternative treatments help alleviate the symptoms of the disease. Such treatments may include acupuncture, ingestion of wheatgrass juice, aloe vera gel, omega-3 fish oil, various probiotics, curcumin, and fecal microbiota transplantation.
Several articles highlight the efficacy of probiotics in preventing inflammation and maintaining remission in individuals with colitis. Probiotics act as a barrier, lining the intestinal tract and preventing other luminal bacteria from penetrating the mucosal lamina propria through competitive inhibition, while stimulating the mucosal immune system.
Probiotics also enhance mucus production, which protects against invasive bacteria, induces protective cytokines, suppresses pro-inflammatory cytokines, and can modulate the intestinal immune system.
In turn, fecal microbiota transplantation (FMT) — transferring stool from a healthy donor to a patient with UC — is a promising approach to alleviate the severity of UC. FMT has been shown to increase secretory IgA and mucin production, as well as the production of antimicrobial peptides.
FAQ
1. How does ulcerative colitis differ from Crohn’s disease?
Ulcerative colitis affects only the colon and only the mucosal layer. Crohn’s disease can occur in any part of the GI tract and damages all layers of the intestinal wall.
2. Is ulcerative colitis hereditary?
There is a genetic predisposition (the risk is 4 times higher if close relatives are affected).
3. Can ulcerative colitis be cured permanently?
It is a chronic disease. Modern therapy can achieve many years of remission, where a person lives a full life. Surgical removal of the entire colon is technically considered a “cure” of intestinal symptoms of UC, but it is quite traumatic and a substantial intervention.
4. How long does a flare-up of ulcerative colitis last?
The duration depends on the severity. Mild forms resolve in 2–4 weeks, while severe ones may require hospitalization and months to achieve full remission.
5. Can ulcerative colitis progress to cancer?
The risk of colorectal cancer increases with a disease duration of more than 8–10 years. Such patients need to undergo colonoscopy annually for early detection of precancerous changes.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Achkasov SI, Shapina MV, Veselov VV, et al. Prediktory kolektomii u patsientov so sverkhtyazhelym yazvennym kolitom [Predictors of colectomy in patients with super-severe ulcerative colitis]. Koloproktologiya [Coloproctology]. 2020;19(3):37-48. Russian. doi: 10.33834/2073-7564-2020-19-3-37-48.
3.
Belousova EA, Nikitina NV, Tsodikova OM. Lechenie yazvennogo kolita legkogo i sredneyazhelogo techeniya [Treatment of mild and moderate ulcerative colitis]. Farmateka. 2013;(2):42-46. Russian.
4.
Ivashkin VT, Lapina TL, editors. Gastroenterologiya. Natsional’noe rukovodstvo [Gastroenterology. National guidelines]. Moscow: GEOTAR-Media; 2008. 704 p. Russian. ISBN 978-5-9704-0675-5.
5.
Knyazev OV, Zvyaglova MY, Kagramanova AV, et al. Poterya otveta i chastota nezhelatel’nykh yavleniy u patsientov s yazvennym kolitom i bolezn’yu Krona pri perekhode s original’nogo preparata infliksimab na ego biosimilyary [Loss of response and the rate of adverse events in patients with ulcerative colitis and Crohn’s disease when switching from the originator infliximab to its biosimilars]. Ter Arkh. 2021;93(2):150-157. Russian. doi: 10.26442/00403660.2021.02.200613. PMID: 36856403.
6.
Khalif IL. Lechebnaya taktika pri yazvennom kolite [Therapeutic tactics for ulcerative colitis]. Rossiyskiy Zhurnal Gastroenterologii, Gepatologii, Koloproktologii [Russian Journal of Gastroenterology, Hepatology, Coloproctology]. 2006;16(3):58-62. Russian.
7.
Chashkova EY, Vladimirova AA, Neustroev VG, et al. Vospalitel’nye zabolevaniya tolstoy kishki — aspekty diagnostiki [Inflammatory bowel diseases — aspects of diagnostics]. Byulleten’ Vostochno-Sibirskogo Nauchnogo Tsentra SO RAMN [Bulletin of the Eastern-Siberian Scientific Center of the SB RAMS]. 2011;(4 Pt 2):209-211. Russian.
8.
Annese V, Daperno M, Rutter MD, et al. European evidence-based consensus for endoscopy in inflammatory bowel disease. Journal of Crohn’s and Colitis. 2013;7(12):982–1018.
9.
Cherfane CE, Gessel L, Cirillo D, Zimmerman MB, Polyak S. Monocytosіs and a Low Lymphocyte to Monocyte Ratio as Effective Biomarkers of Ulcerative Colitis Disease Activity. Inflamm Bowel Dis. 2015 Aug;21(8):1769–75.
10.
Collins P, Rhodes J. Ulcerative colitis: diagnosis and management. BMJ. 2006 10;333(7563):340–3.
11.
Coskun M. Intestinal epithelium in inflammatory bowel disease. Front Med. 2014;1:24.
12.
Fernández-Clotet A, Castro-Poceiro J, Panés J. Tofacitinib for the treatment of ulcerative colitis. Expert Rev Clin Immunol. 2018;14(11):881–92.
13.
Kiela PR, Ghishan FK. Physiology of intestinal absorption and secretion. Best Pract Res Clin Gastroenterol. 2016;30(2):145-59.
14.
Mak WY, Zhao M, Ng SC, Burisch J. The epidemiology of inflammatory bowel disease: east meets west. J Gastroenterol Hepatol. 2019.
15.
M’koma AE. Inflammatory bowel disease: an expanding global health problem. Clinical Medicine Insights. Gastroenterology. 2013;6(CGast):S12731.
16.
Yamamoto-Furusho JK, Sánchez-Osorio M, Uribe M. Prevalence and factors associated with the presence of abnormal liver function tests in patients with ulcerative colitis. Ann Hepatol. 2010 Oct-Dec;9(4):397–401.