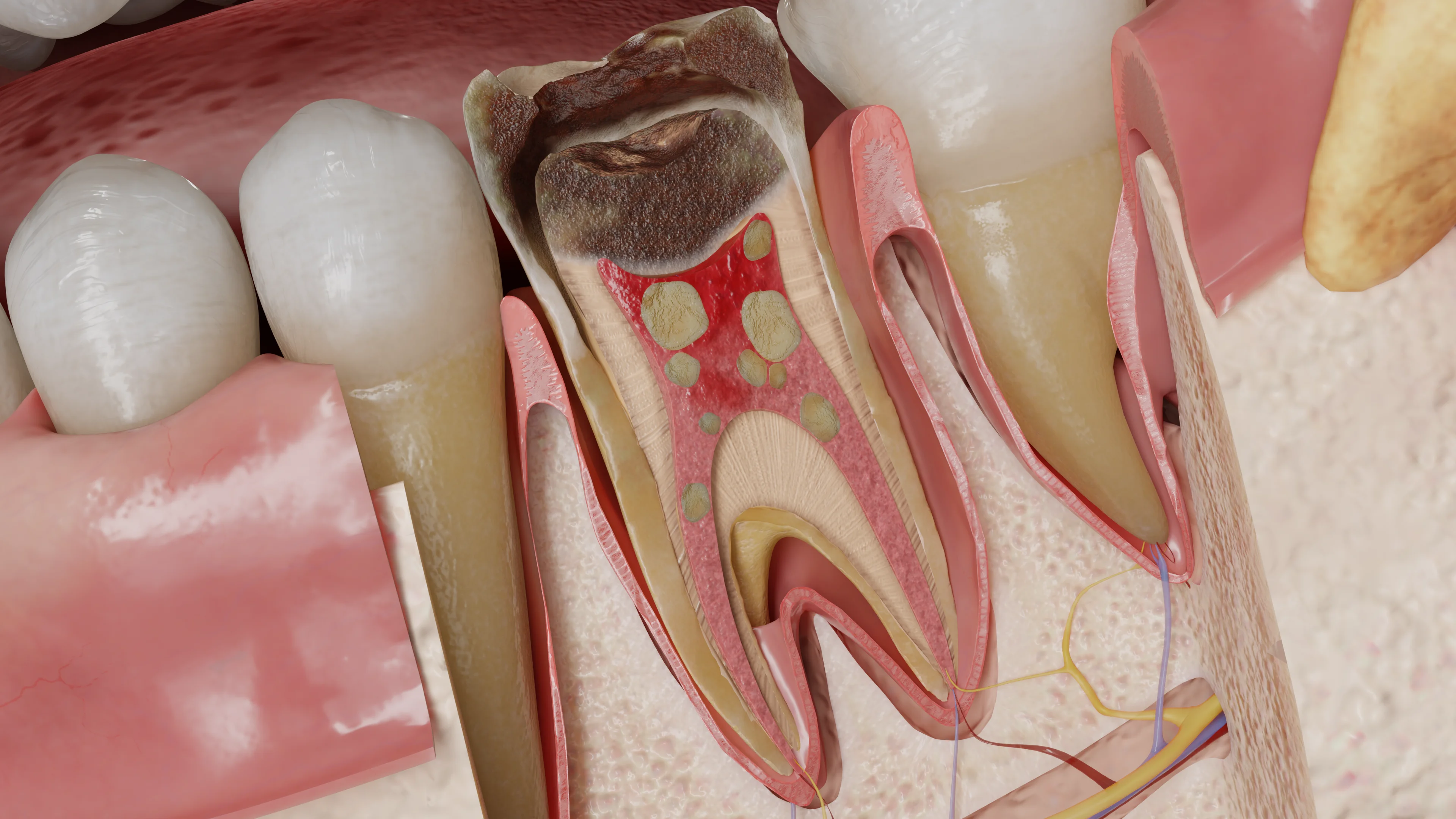
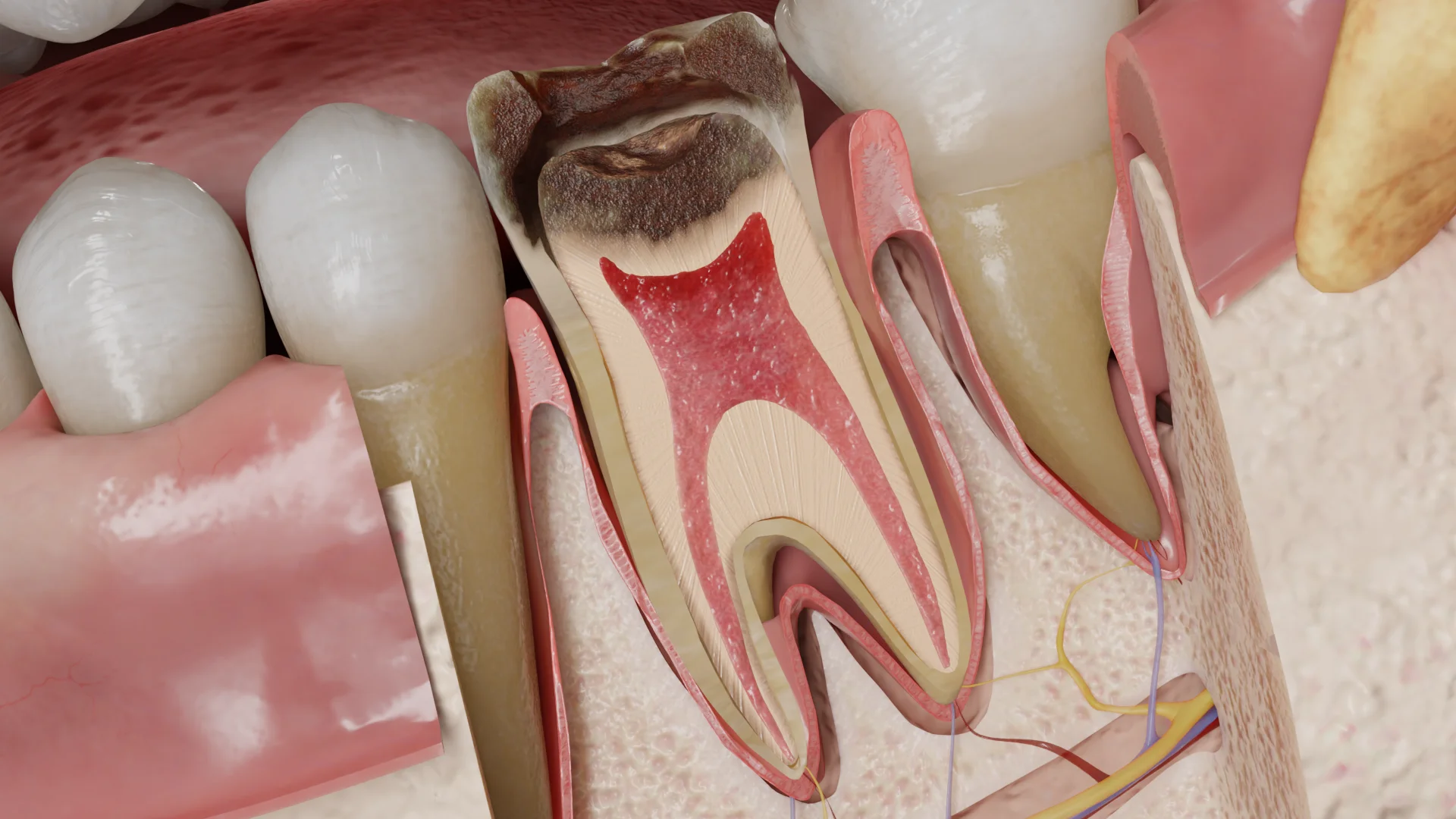
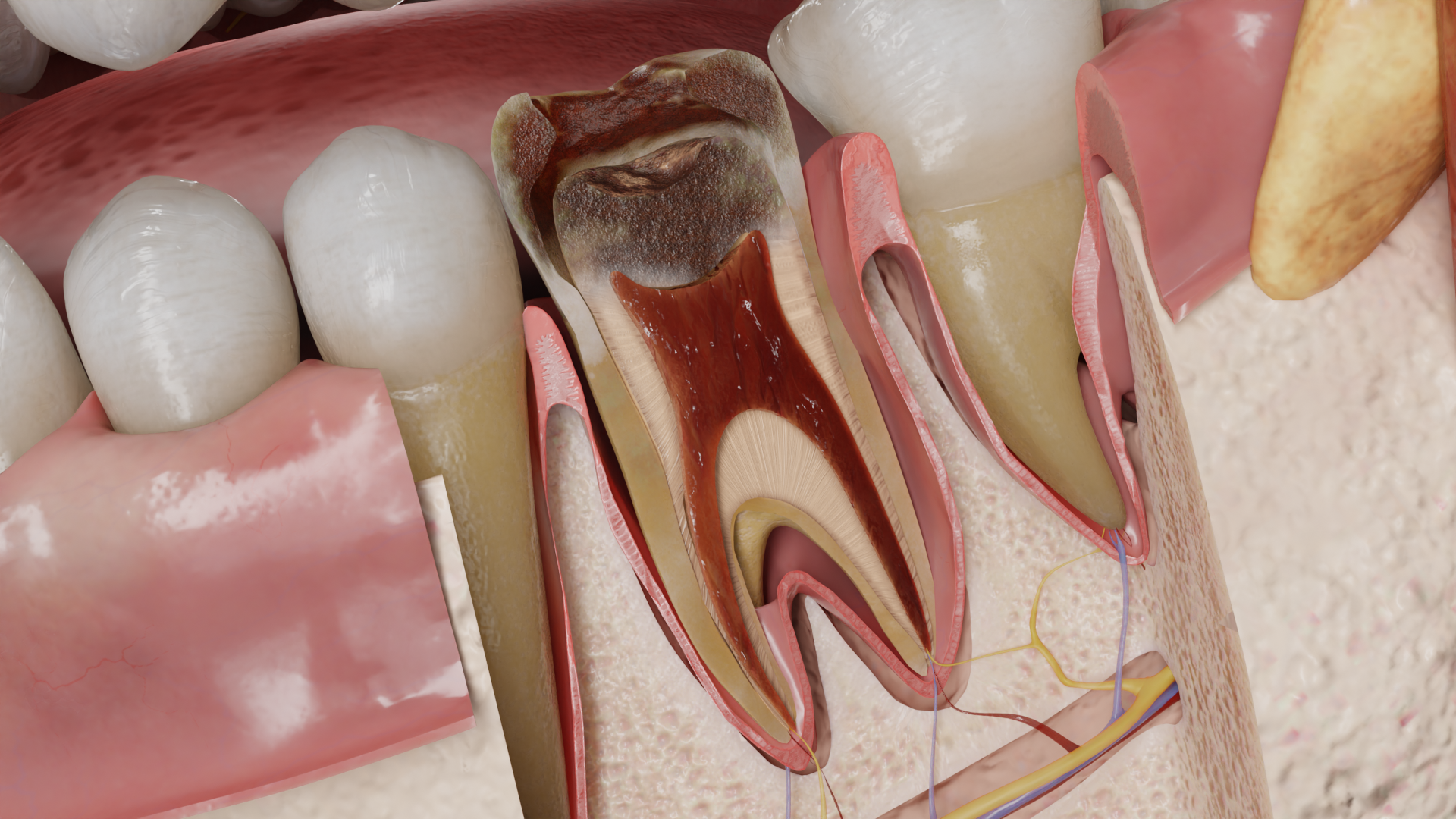
Systemic Enamel Hypoplasia: Etiology, Classification, Clinical Presentation, and Treatment
Developmental Enamel Defects: Systemic Hypoplasia. Overview of the Etiology, Clinical Forms, Diagnosis, and Aesthetic Restoration Techniques for Teeth.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Myiasis is a parasitic disease caused by fly larvae from the order Diptera, which lay eggs in human or animal tissues.
Oral myiasis is a subgroup of myiases, characterized by the involvement of oral cavity tissues. The condition is rare, and adequately assessing its prevalence is challenging. In general, the literature cites isolated cases. Between 1990 and 2020, 157 cases of oral myiasis were reported in English-language literature (based on PubMed, Ovid, Web of Science, Scopus, and LILACS). The disease is most prevalent among low-income populations in tropical regions. It develops due to parasite invasion in untreated open wounds of the oral cavity.
Predisposing factors include:
To lay eggs, an adult female fly searches for accumulations of decomposing organic matter, which can be represented by an untreated wound in the oral cavity. Adult female flies instinctively lay eggs where a less mobile larva will be provided with a sufficient amount of food.
Depending on the fly species, the eggs hatch within 8–24 hours, and the resulting larvae start feeding on surrounding tissues, causing both mechanical and physical damage due to toxins that destroy host tissues. The larvae complete their development within 5–7 days, then crawl out of the wound and fall to the ground to pupate.

Patients complain of:
The clinical presentation primarily depends on the localization of the affected area by larvae. For instance, when the parasite is localized in the wound area of the upper lip, facial asymmetry will be observed due to collateral edema of the soft tissues of the upper lip. Whereas when the inflammatory process is localized in the hard palate area, the configuration of the face will not be altered.
Common signs and symptoms of the affected area include:
When secondary infection occurs, purulent discharge from the affected area and a putrid odor may also be observed. Regional lymph nodes (often submandibular) may be enlarged, mobile, soft, painful/slightly painful on palpation.
Direct visualization of white/creamy larvae and/or eggs.

CT of the maxillofacial area, if deeper spread into the soft tissues is suspected (rare).
The diagnosis is primarily based on the visualization of larvae or parasitic eggs in the patient’s wound!
Find more scientifically accurate content on our social media








Due to the rarity and low social significance of the disease, there are no universally accepted treatment protocols. Among the agents used for treatment, four groups can be conditionally distinguished:
Depending on the neglecting of the process, additional interventions are recommended:
1. What is oral myiasis?
2. Is oral myiasis contagious?
3. Can a healthy person contract it in their sleep?
4. What consequences can the disease lead to if untreated?
References:
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Passos JBSD, Coelho LV, De Arruda JAA, De Oliveira Silva LV, Valle IBD, De Souza Santos M, De Figueiredo EL, Abreu LG, Mesquita RA. Oral myiasis: Analysis of cases reported in the English literature from 1990 to 2020. Special Care in Dentistry [Internet]. 2020 Oct 30;41(1):20–31.
Available from: https://pubmed.ncbi.nlm.nih.gov/33125723/
3.
Francesconi F, Lupi O. Myiasis. Clin Microbiol Rev. 2012;25(1): 79-105.
4.
Hall MJR. Traumatic myiasis of humans in the Old World. In: Service MW, ed. Encyclopedia of Arthropod-transmitted Infections. 2001: 363-375.
5.
WHO. Guidelines for the management of myiasis. 2020 update.
6.
Costa DC, et al. Oral myiasis: a systematic review of 128 cases. J Oral Maxillofac Surg. 2021;79(8): 1655-1664.
7.
Zumpt F. Myiasis in Man and Animals in the Old World. London: Butterworths; 1965.
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io