Fetal Positions in the Womb: Types, Diagnosis, Risks, Labor Management Techniques
Daria G.Gynecologist, fertility specialist, MD
17 min read·August 05, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
The fetal position is defined as the relationship between the axis of the fetal body and the longitudinal axis of the uterus. The fetal position is defined as one of the following:
Longitudinal: when the axes are parallel (optimal);
Transverse: when positioned perpendicularly (pathological);
Oblique: when forming an acute angle with the uterine axis (pathological).
The optimal fetal presentation is the occiput anterior presentation with a well-flexed head facing anteriorly, where the fetal body is aligned longitudinally with the uterine axis.
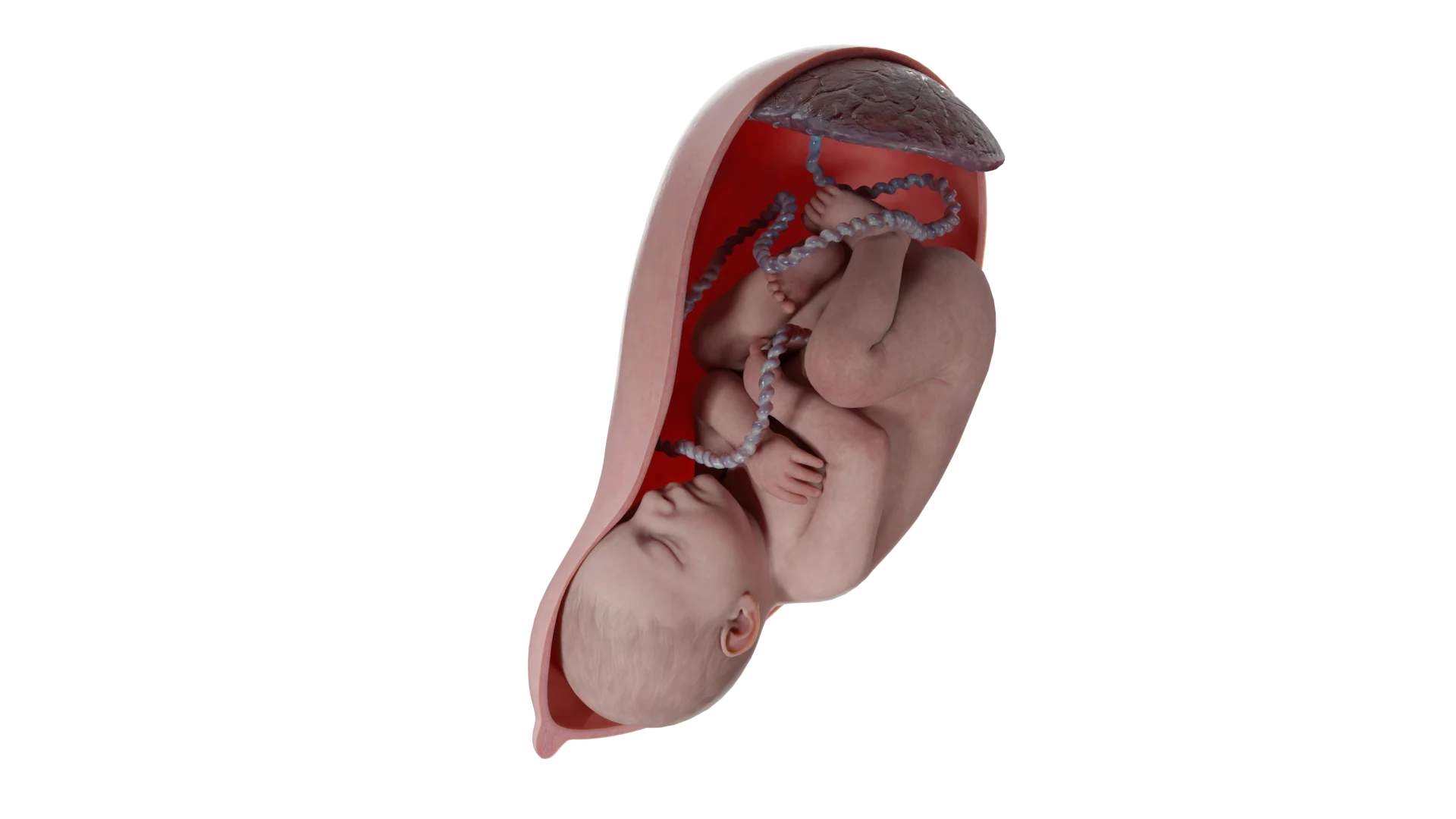
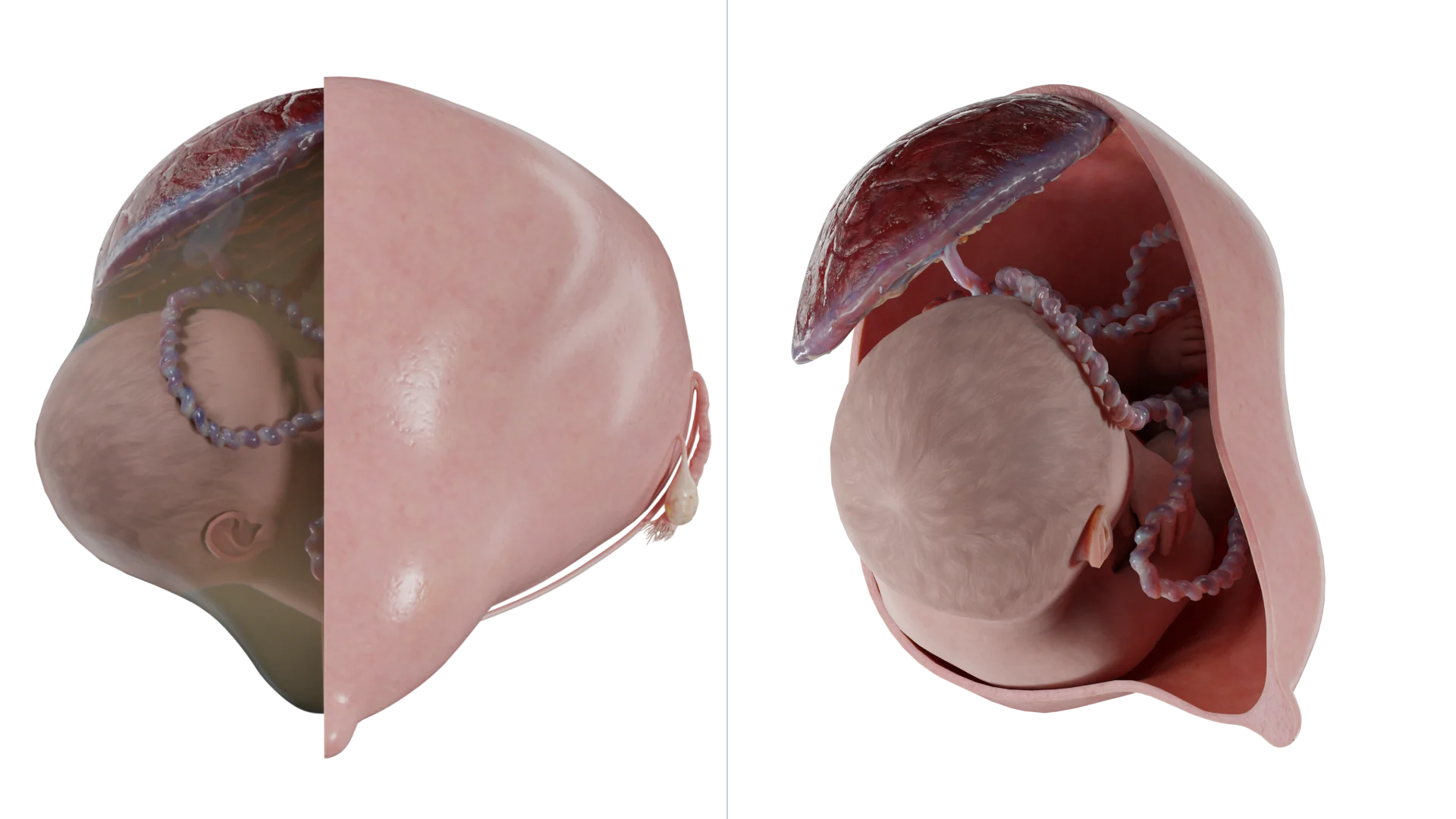
3D animation: transverse fetal position in the uterus
Transverse position is diagnosed when the fetus is positioned perpendicularly to the longitudinal axis of the uterus. Two configurations exist:
The curvature of the fetal spine is oriented downward (also known as dorsoinferior), with the fetal shoulder close to the cervix;
The curvature of the fetal spine is oriented upward (referred to as dorsosuperior); the smaller parts of the fetus and the umbilical cord are near the cervix.
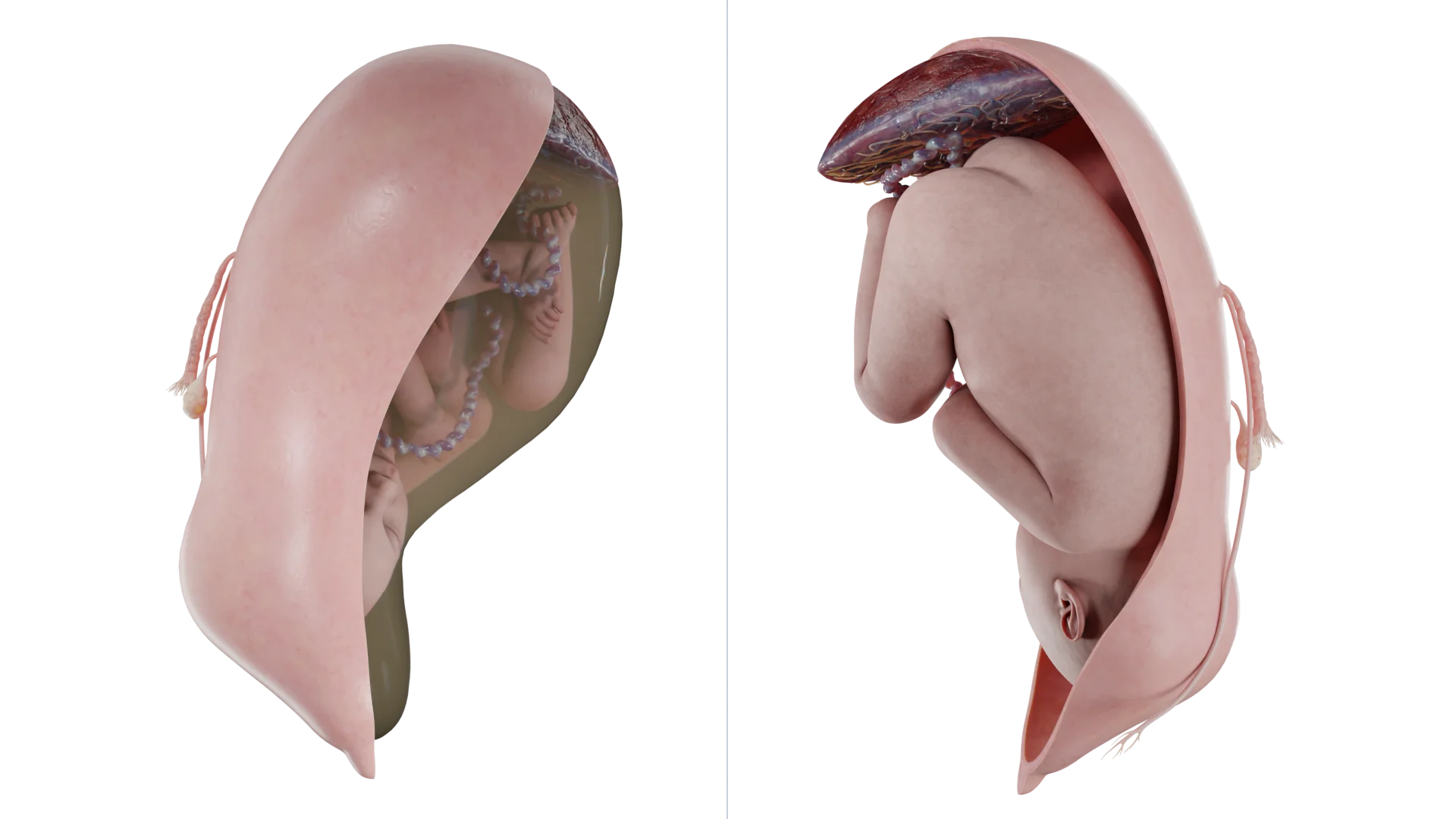
3D animation: oblique fetal position in the uterus
If the fetus is in an oblique lie, its body and the axis of the uterus are positioned at an acute angle, with the pelvic or cephalic pole located below the iliac crest. Upon palpation and using Leopold’s maneuvers, the presenting part of the fetus cannot be felt above the symphysis. Fetal heartbeat auscultation is conducted around the navel area. The oblique fetal position is highly unstable and often changes to a longitudinal or transverse position during labor.
In transverse and oblique positions, the first position is determined if the fetal head is on the left, and the second if the head is on the right. Anterior view is determined when the back faces the anterior uterine wall, and posterior when the back faces the posterior wall.
Incidence
Transverse and oblique fetal positions during labor are diagnosed in approximately 1 in 300 cases. Improper fetal positioning is usually identified in early pregnancy. It’s important to note that the transverse fetal position is unstable: according to literature, 85% of cases diagnosed at 24–28 weeks change to longitudinal by term.
Pathogenesis and risk factors
In early pregnancy, when the volume of amniotic fluid is large relative to fetal mass, the fetus is not restricted by the size of the uterine cavity and often assumes an incorrect position. As pregnancy progresses, the amniotic fluid volume decreases relative to fetal size, and the fetus often assumes a longitudinal position parallel to the uterine body axis along the gravity line.
Premature labor is the most common risk factor for transverse fetal position during labor. Other risk factors include multiple gestation, placenta previa, anatomically narrow pelvis, uterine abnormalities or tumors, polyhydramnios, and fetal abnormalities. The site of placental implantation, uterine anatomical deformities, and uterine stretching alter the uterine cavity space and likely affect fetal positioning.
Diagnosis
At the initial examination, attention is drawn to the abnormal abdominal configuration with increased transverse dimensions of the uterus and abdominal circumference.
The diagnosis may be based on abdominal palpation combined with Leopold’s maneuvers. It is not possible to palpate the fetal head above the symphysis. Further palpation reveals the fetal head along the right or left uterine margin. Determining whether the fetal buttocks are directed upward or downward is more difficult, especially in obese patients. The sensitivity of abdominal palpation for detecting abnormal fetal positioning at 35–37 weeks of gestation is approximately 70%.
Ultrasound
Ultrasound (US) examination is used to confirm the diagnosis and determine the exact fetal position and presentation.
In cases of deviations, the anatomy of the uterus and fetus should be examined for any anomalies or conditions associated with the unstable lie. First and foremost, placenta previa must be ruled out. It is important to note that if a transverse fetal lie is suspected based on palpation and ultrasound is unavailable, it is recommended to refrain from performing a digital vaginal examination.
Complications
Despite significant reductions in morbidity and mortality associated with transverse fetal positioning due to modern perinatal care, this category of pregnant women still has an increased risk of maternal and perinatal morbidity compared to women with a longitudinal fetal position.
Complications largely depend on the accessibility and quality of healthcare services in the country. For example, in developed countries with unrestricted access to ultrasonography and qualified care, the main complications are as follows:
Placenta previa;
Umbilical cord prolapse;
Fetal trauma;
Fetal malformations;
Premature birth.
In resource-limited countries, maternal and perinatal morbidity and mortality remain high where ultrasonography, emergency cesarean sections, and neonatal intensive care are unavailable. Uterine rupture from prolonged labor with a transverse fetal position is the main cause of maternal and perinatal mortality.
During labor, the transverse fetal position can lead to:
Prolapse of fetal parts;
Prolapse of the umbilical cord;
Advanced transverse lie.
An advanced transverse fetal position forms due to increasing uterine contractile strength, during which the fetus loses mobility, its arm or umbilical cord may prolapse, and in severe cases, shoulder impaction occurs.
Labor management
The oblique position often progresses to a transverse position, and a transverse fetal position is an indication for delivery by cesarean section. The mode of delivery also depends on the clinical circumstances at the time of diagnosis. Important factors to consider include:
Position of the placenta and umbilical cord;
Gestational age and fetal viability;
Onset of labor or rupture of membranes;
Multiple pregnancies.
External obstetric version for transverse fetal position
When a transverse fetal lie has been identified before the labor onset, and there are no other contraindications to vaginal birth, external cephalic version (ECV) should be attempted between Weeks 37 and 37.6 of pregnancy.
Since the amniotic fluid volume is greatest during this period, and the uterine tone and fetal weight are less than at later stages, performing the procedure at 37–37.6 weeks increases the likelihood of success.
Expert opinions vary on the impact of maternal weight, placental position, and amniotic fluid volume on procedure success. Most practitioners believe that repeated motherhood, a normal weight, a posterior placenta, and sufficient amniotic fluid increase the chance of a successful version. Additionally, if complications arise during the attempt, the procedure may be concluded with an emergency cesarean section. If the initial version attempt fails, the procedure is repeated at 38–39 weeks of pregnancy.
An alternative approach involves performing an external obstetric version at 39 weeks, followed by amniotomy and induction of labor. The rationale for labor induction is that the transverse position is extremely unstable and can spontaneously revert after the version, unlike breech presentation, when reversion is rare.
Risks associated with the procedure
The most common complication is a temporary decrease in fetal heart rate (up to 40% of cases). This condition may persist for several minutes after the procedure and is not associated with adverse effects on the fetus. Rare complications include fetal bone fractures, premature rupture of the membranes, placental abruption (if the placenta is normally located), hemorrhage, and uterine laceration. Currently, there are not enough studies to show whether the overall risk of perinatal mortality increases following external cephalic version (ECV). A 2015 Cochrane review reported that the risk of perinatal death among ECV patients was 2 out of 644 cases compared to 6 out of 661 cases among women who did not undergo the procedure.
Procedure methodology
Prior to the procedure, an ultrasound is conducted to determine fetal position, weight, and the volume of amniotic fluid, as well as to rule out placenta previa and fetal abnormalities. A non-stress test (alternatively, a biophysical profile) should be conducted prior to the manipulation. The procedure is performed in a fully equipped surgery room, with the mandatory presence of anesthesiologists/intensivists. Routine tocolysis and the routine use of spinal or epidural anesthesia are not recommended.
External cephalic version involves gently moving the fetal cephalic end towards the woman’s pelvis while shifting the pelvic end towards the uterine fundus. There is no consensus on the number of external cephalic version attempts that can be performed. After an attempt, regardless of its success, a non-stress test (biophysical profile if needed) should be repeated. Additionally, Rh-negative women should be administered Rh immune globulin.
Managementin various clinical
situations
Premature birth
Premature labor in a transverse fetal position necessitates a cesarean section.
Premature rupture of membranes
If the gestational age exceeds 34 weeks, delivery should be carried out via cesarean section. If the gestational age is less than 34 weeks, it is recommended to adopt a watchful waiting strategy, which includes preventive measures for fetal respiratory distress syndrome. It’s important to note that watchful waiting is only possible in the absence of infection, bleeding, or labor activity.
Transverse position of the second fetus after the birth of the first fetus
After the delivery of the first fetus, the second may assume a transverse position, regardless of its initial intrauterine position.
In such cases, an internal version can be performed under anesthesia. This procedure is carried out immediately after the delivery of the first fetus, when the cervix is fully dilated and the membranes remain intact. The procedure should only be performed by an experienced physician, as there is a risk of fetal injury in complex cases. External obstetric rotation is an alternative approach that is easier to perform. Regardless of the procedure, ultrasound guidance is mandatory to monitor fetal status.
No studies in the literature provide high-quality comparative data demonstrating the relative merits of internal versus external versions. It is crucial to note that a physician should act based on their level of training and experience.
Antenatal death
In cases of antenatal fetal death with a transverse position, ECV should be performed regardless of membrane integrity, followed by labor induction.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Specifics of cesarean section
In patients with a well-developed lower uterine segment, a low transverse hysterotomy is performed. Some experts recommend a vertical uterine incision, which is also a reasonable approach if the lower uterine segment is underdeveloped. However, vertical hysterotomy, even when limited to the lower segment, is less desirable because performing a vertical incision increases the risk of uterine rupture in subsequent pregnancies. Prior to surgery, performing external cephalic version is recommended to facilitate extraction. The fetal part that is to become the presenting one is turned towards the inlet of the woman’s pelvis, while the opposite end is pointed in the opposite direction. The fetus can be rotated to a cephalic or breech presentation; however, most physicians prefer a breech presentation because it is technically easier to perform. After completion of the version, a medical assistant holds the fetus in the longitudinal position to prevent it from reverting to the original position. Once the hysterotomy is performed, the fetus is extracted.
FAQ
1. How to determine fetal position?
Fetal position is determined through clinical examination and instrumental methods. During abdominal palpation (Leopold’s maneuvers), the physician evaluates the position of the fetal head, back, and buttocks. Ultrasound is the most precise method for confirming fetal position and presentation, helping exclude associated health conditions. In cases of oblique or transverse position, fetal heartbeats are usually auscultated at the umbilical region.
2. How does a transverse fetal position differ from an oblique one?
In a transverse position, the fetal axis is strictly perpendicular to the uterine axis — the fetus is positioned horizontally, with its head and pelvic end at the sides of the uterus. An oblique position is characterized by an acute angle between the fetal and uterine axes, with one end of the fetus (either cephalic or pelvic) located below the iliac crest. An oblique position is less stable and often converts to a longitudinal or transverse position during labor.
3. What are the causes of abnormal fetal position?
The main causes include preterm labor when the fetus does not have time to assume the correct position. Other factors: multiple pregnancy, placenta previa, uterine structure abnormalities, polyhydramnios, and contracted pelvis. Risk increases with uterine tumors or fetal development abnormalities that limit its mobility.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
American College of Obstetricians and Gynecologists. Mode of term singleton breech delivery (Practice Bulletin No. 221). Obstet Gynecol. 2023;141(5):e156-e171.
3.
Hankins GDV, et al. Transverse fetal lie: diagnosis, risks, and management. Am J Obstet Gynecol. 2020;222(3):S1-S8.
4.
Royal College of Obstetricians and Gynaecologists. External cephalic version and reducing the incidence of term breech presentation (Green-top Guideline No. 20a). 2023.
5.
Hofmeyr GJ, et al. External cephalic version for term breech presentation. Cochrane Database Syst Rev. 2023;2023(4):CD000083.
6.
Ultrasound-guided management of transverse lie in late pregnancy. Ultrasound Obstet Gynecol. 2023;61(2):210-215.
7.
Bianco A, et al. Management of transverse fetal lie in the third trimester: a systematic review and meta-analysis. Am J Obstet Gynecol MFM. 2024;6(1):101012. doi: 10.1016/j.ajogmf.2024.101012.
8.
Zafarmand MH, et al. Ultrasound-guided management of unstable lie in late pregnancy: a multicenter randomized trial. Ultrasound Obstet Gynecol. 2023;61(3):345-351. doi: 10.1002/uog.26145.
Gerson KD, Loder A, Landau Z, Anton L. Xenobiotic metabolites modify immune responses of the cervicovaginal epithelium: potential mechanisms underlying barrier disruption. BJOG an International Journal of Obstetrics & Gynaecology [Internet]. 2023 Sep 13;131(5):665–674.
Available from: https://doi.org/10.1111/1471-0528.17654
11.
D’Souza R, et al. Maternal and neonatal outcomes in pregnancies complicated by transverse lie: systematic review. Eur J Obstet Gynecol Reprod Biol. 2023;287:56-62. doi: 10.1016/j.ejogrb.2023.05.038.