Hypothyroidism: Classification, Clinical Presentation, Diagnosis, and Treatment
Hypothyroidism is a condition characterized by a deficiency of thyroid hormones. Symptoms, diagnosis, and treatment of congenital and acquired forms.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hematology
Hematopoiesis and blood-related disorders
Hepatology
Liver, gallbladder, and biliary tract diseases
Histology
Microscopic tissue and cell structures
Infectious diseases
Bacterial, viral, and parasitic infections
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Orthopedics
Bone, joint, and soft tissue disorders
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
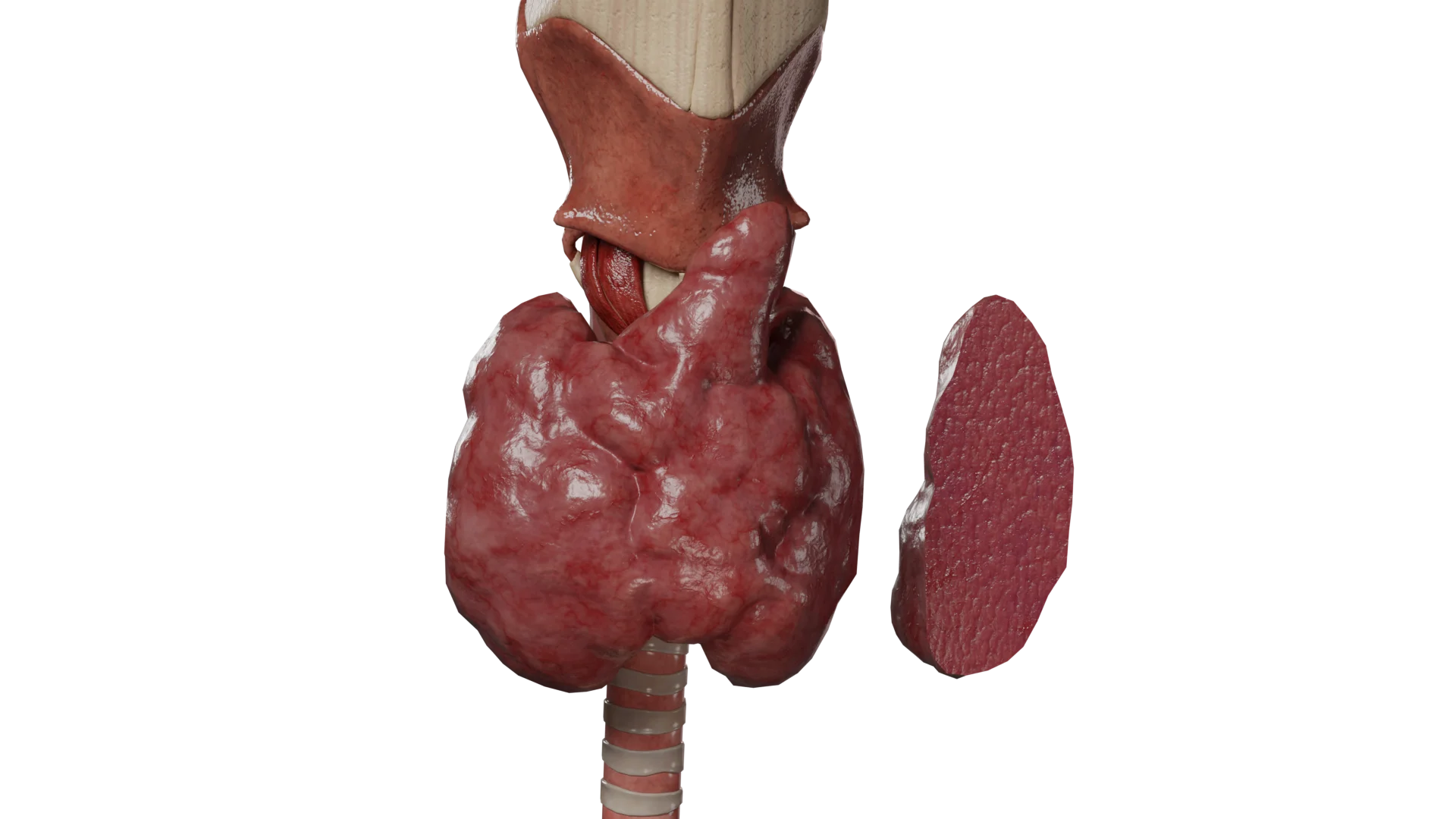
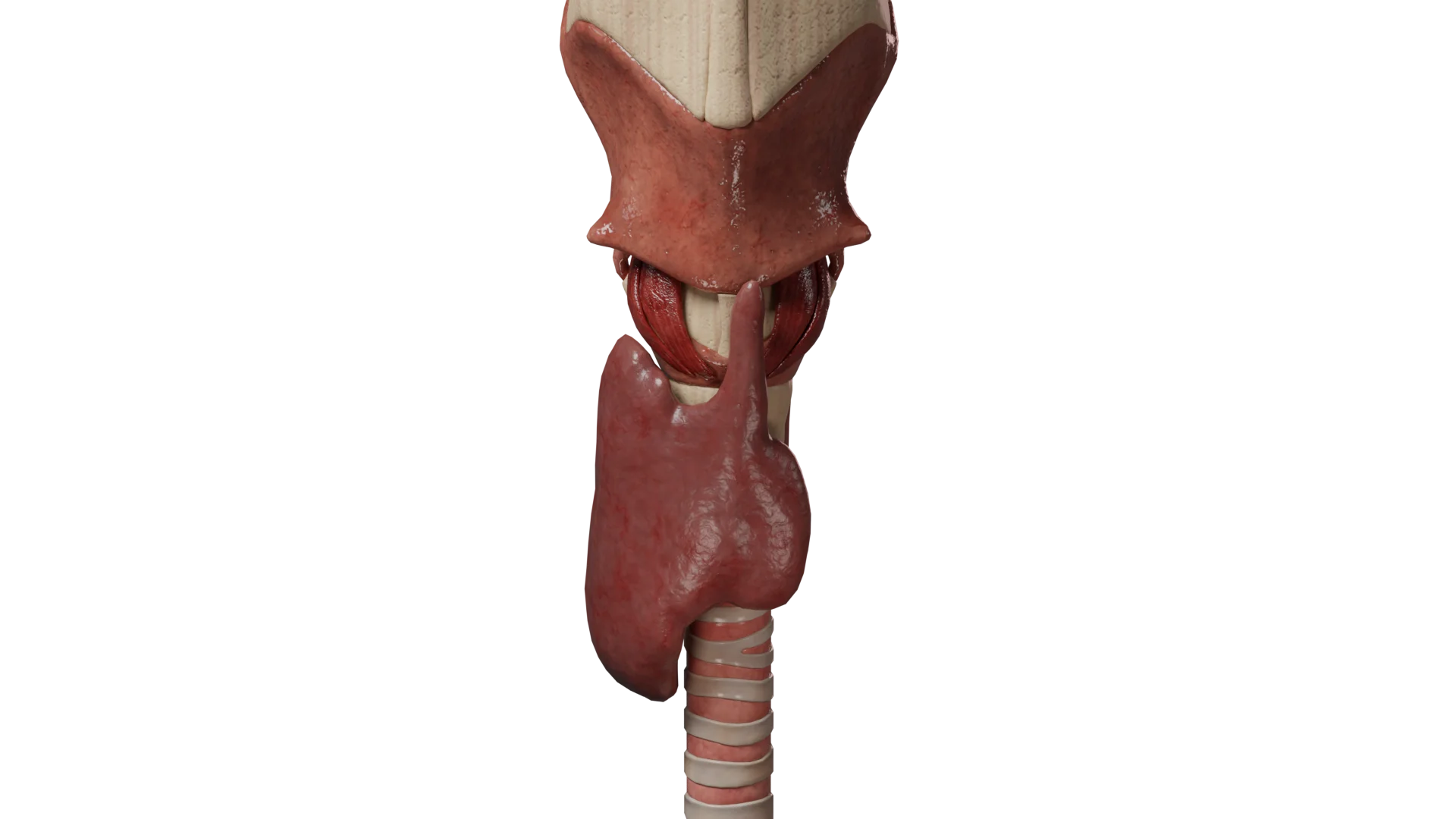
Hyperparathyroidism is an endocrine disorder caused by the excessive production of parathyroid hormone, leading to disorder of the calcium-phosphate metabolism and the development of hypercalcemia, osteopenia, renal dysfunction, and cardiovascular system impairments. It is the third most common endocrine disease (after diabetes mellitus and thyroid diseases), more frequently observed in women.
3D models of hyperparathyroidism variants:
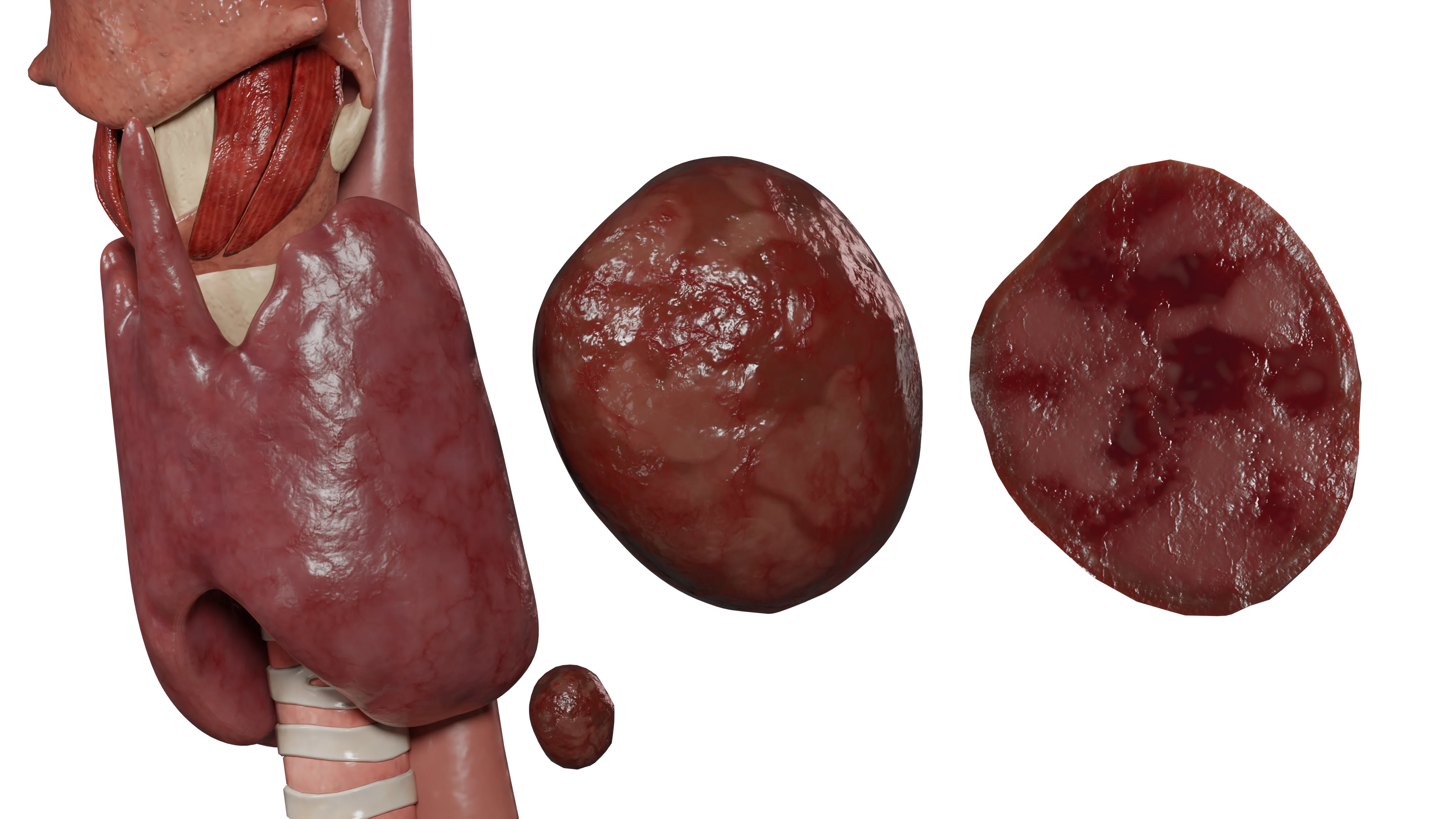 Primary hyperparathyroidism
Primary hyperparathyroidism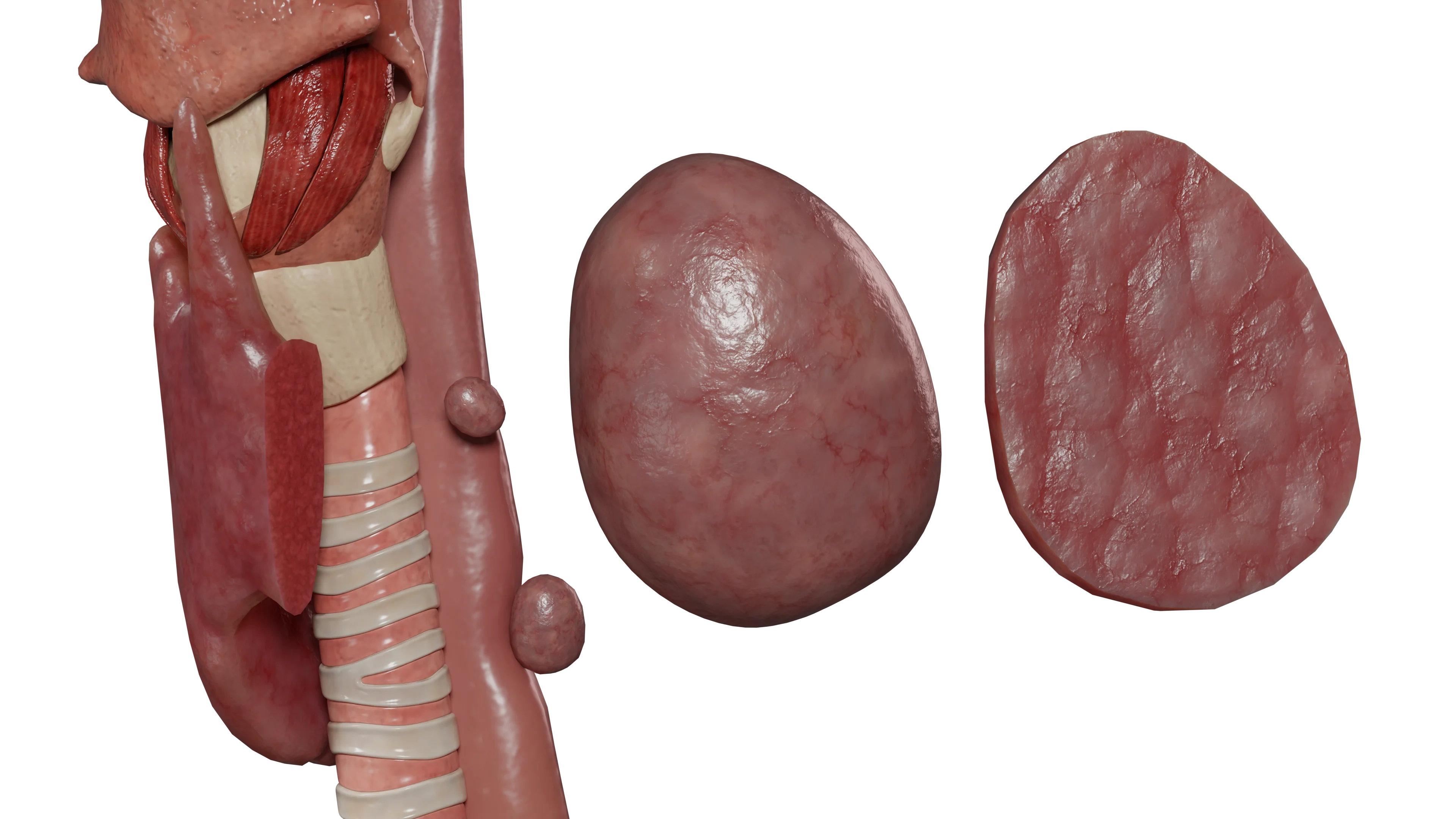 Secondary hyperparathyroidism
Secondary hyperparathyroidism Tertiary hyperparathyroidism
Tertiary hyperparathyroidismDepending on the cause:
Classification by clinical course:
Primary hyperparathyroidism is a condition characterized by increased production of parathyroid hormone.
In the overwhelming majority of cases (80-85%), it is caused by an adenoma of one of the parathyroid glands. Less commonly, parathyroid gland hyperplasia and parathyroid gland carcinoma occur (less than 1%). It develops due to pathology of, most frequently, one of the parathyroid glands.
Parathyroid gland adenoma is characterized by the development of functional autonomy, leading to increased parathyroid hormone production.
Parathyroid gland adenoma can be sporadic or genetically determined (up to 10% of cases).
Parathyroid gland adenoma may occur in the following hereditary syndromes:
Parathyroid hormone plays a crucial role in calcium-phosphate metabolism through the following mechanisms:
Furthermore, parathyroid hormone inhibits the reabsorption of phosphorus by the renal tubules, leading to hyperphosphaturia. This mechanism maintains serum phosphorus levels within or below the normal range.
In patients with primary hyperparathyroidism, the effect of increased calcium reabsorption may be offset by elevated hypercalcemia. In such cases, hypercalciuria will be detected.
Thus, patients with primary hyperparathyroidism are characterized by the following:
Secondary hyperparathyroidism develops in the context of chronic kidney disease (CKD) as a compensation for prolonged hypocalcemia.
Its development involves the following mechanisms:
The aforementioned mechanisms result in continuous stimulation of the parathyroid glands’ function and, as a consequence, hyperplasia development.
Thus, secondary hyperparathyroidism is characterized by:
Tertiary hyperparathyroidism develops in association with long-term secondary hyperparathyroidism, leading to adenomatous transformation of the parathyroid glands with the development of functional autonomy.
Tertiary hyperparathyroidism is characterized by:
Hyperparathyroidism can occur in three variants:
Currently, in the majority of cases, hyperparathyroidism is detected in the subclinical form through routine clinical and laboratory studies, and patients do not report any complaints at the time of diagnosis.
Early symptoms of hyperparathyroidism are nonspecific. These include:
Long-standing hyperparathyroidism leads to the development of osteoporosis, the symptoms of which are:
In addition to osteoporosis manifestations, hyperparathyroidism is characterized by the following symptoms caused by prolonged hypercalcemia:
A hyperparathyroid (or hypercalcemic) crisis is a life-threatening condition that develops in patients against a background of pre-existing hyperparathyroidism. Characterized by a rapid sharp increase in serum calcium levels above 3.5 mmol/L, with parathyroid hormone levels generally exceeding the norm by more than 20 times.
Provoking factors for crisis development may include infectious diseases, dehydration, and prolonged immobilization. Mortality ranges from 60 to 90% and requires immediate therapy in intensive care units.
Symptoms of hyperparathyroid crisis:
Main examination methods:
In a blood biochemistry, levels of parathyroid hormone, calcium (total and ionized), phosphorus, alkaline phosphatase (increased due to bone resorption), and vitamin D should be determined. Additionally, urinary calcium and phosphorus excretion levels are assessed (daily urine test).
Dynamic laboratory indicators for various variants of hyperparathyroidism:
| Serum indicators | Primary hyperparathyroidism | Secondary hyperparathyroidism | Tertiary hyperparathyroidism |
|---|---|---|---|
| Parathyroid hormone | Elevated | Elevated | Significantly elevated |
| Calcium | Elevated | Normal or decreased | Elevated |
| Phosphorus | Normal or decreased | Elevated | Elevated |
| Alkaline phosphatase | Elevated | Elevated | Elevated |
| Vitamin D | Low | Low | Low |
Imaging methods for parathyroid glands:
Additional examination methods:
Radiological signs characteristic of hyperparathyroidism:
Find more scientifically accurate content on our social media








The main treatment method is surgical. It enables the normalization of parathyroid hormone, calcium, and phosphorus levels in the shortest possible time, thereby reducing the risk of complications.
The operation involves the removal of the adenomatous altered parathyroid gland (parotidectomy), which is the gold standard for the therapy of primary hyperparathyroidism.
After the operation, the development of the “hungry bone” syndrome is possible, which is a persistent (more than 4 days) decrease in serum calcium levels. This syndrome is caused by a sharp decrease in parathyroid hormone levels after surgery, leading to increased osteoblastic activity and capture of calcium and phosphorus for bone tissue formation.
In a biochemical blood test, hypocalcemia, hypophosphatemia, hypomagnesemia, and elevated alkaline phosphatase levels are detected. This syndrome is more common in surgeries for secondary hyperparathyroidism.
Patients who have contraindications to surgical treatment may be assigned conservative therapy in cases of mild hypercalcemia and absence of complications. The following medications are used for the treatment of hyperparathyroidism:
In addition, patients receiving conservative therapy are not advised to restrict dietary calcium intake, as a deficiency in calcium intake may lead to stimulation of the parathyroid glands and an increase in parathyroid hormone levels.
The main treatment method is conservative. Drug therapy is aimed at maintaining and, if possible, normalizing parathyroid hormone, calcium, and phosphorus levels.
In addition to the drugs used in primary hyperparathyroidism, vitamin D receptor activators are also used in the treatment of secondary and tertiary hyperparathyroidism:
If medical therapy is ineffective, surgical treatment is indicated. The extent of surgical intervention is determined individually, based on parathyroid hormone, calcium, phosphorus levels, the overall somatic state of the patient, and the presence of hyperparathyroidism complications.
The following operations can be performed:
Treatment is conducted in an intensive care and resuscitation unit and includes the following:
After stabilization of the condition, surgical treatment is indicated (parathyroidectomy for primary hyperparathyroidism and subtotal or total parathyroidectomy for secondary or tertiary hyperparathyroidism).
1. What is hyperparathyroidism, and what are its consequences?
2. What clinical symptoms of hyperparathyroidism are predominant in women?
3. What laboratory tests are necessary to verify the diagnosis?
4. Is effective conservative therapy possible for primary hyperparathyroidism?
5. Why does secondary hyperparathyroidism develop in the context of kidney disease?
6. What dietary therapy principles should be followed in hyperparathyroidism?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas. VOKA 3D Anatomy & Pathology
Available from: https://catalog.voka.io/
2.
Helbing A, Leslie SW, Levine SN. Primary Hyperparathyroidism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK441895/
3.
Muppidi V, Meegada SR, Rehman A. Secondary Hyperparathyroidism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK557822/
4.
Palumbo VD, Damiano G, Messina M, Fazzotta S, Lo Monte G, Lo Monte AI. Tertiary Hyperparathyroidism: a review. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://pubmed.ncbi.nlm.nih.gov/33956045/
5.
Campos A. Hyperparathyroidism. PubMed [Internet].
Available from: https://radiopaedia.org/articles/hyperparathyroidism
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io