Hyperparathyroidism: Classification, Pathogenesis, Clinical Presentation, Diagnosis, and Treatment
Svetlana D.Surgical oncologist, MD
12 min read·February 12, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Hyperparathyroidism is an endocrine disorder caused by the excessive production of parathyroid hormone, leading to disorder of the calcium-phosphate metabolism and the development of hypercalcemia, osteopenia, renal dysfunction, and cardiovascular system impairments. It is the third most common endocrine disease (after diabetes mellitus and thyroid diseases), more frequently observed in women.
Primary hyperparathyroidism is a condition characterized by increased production of parathyroid hormone.
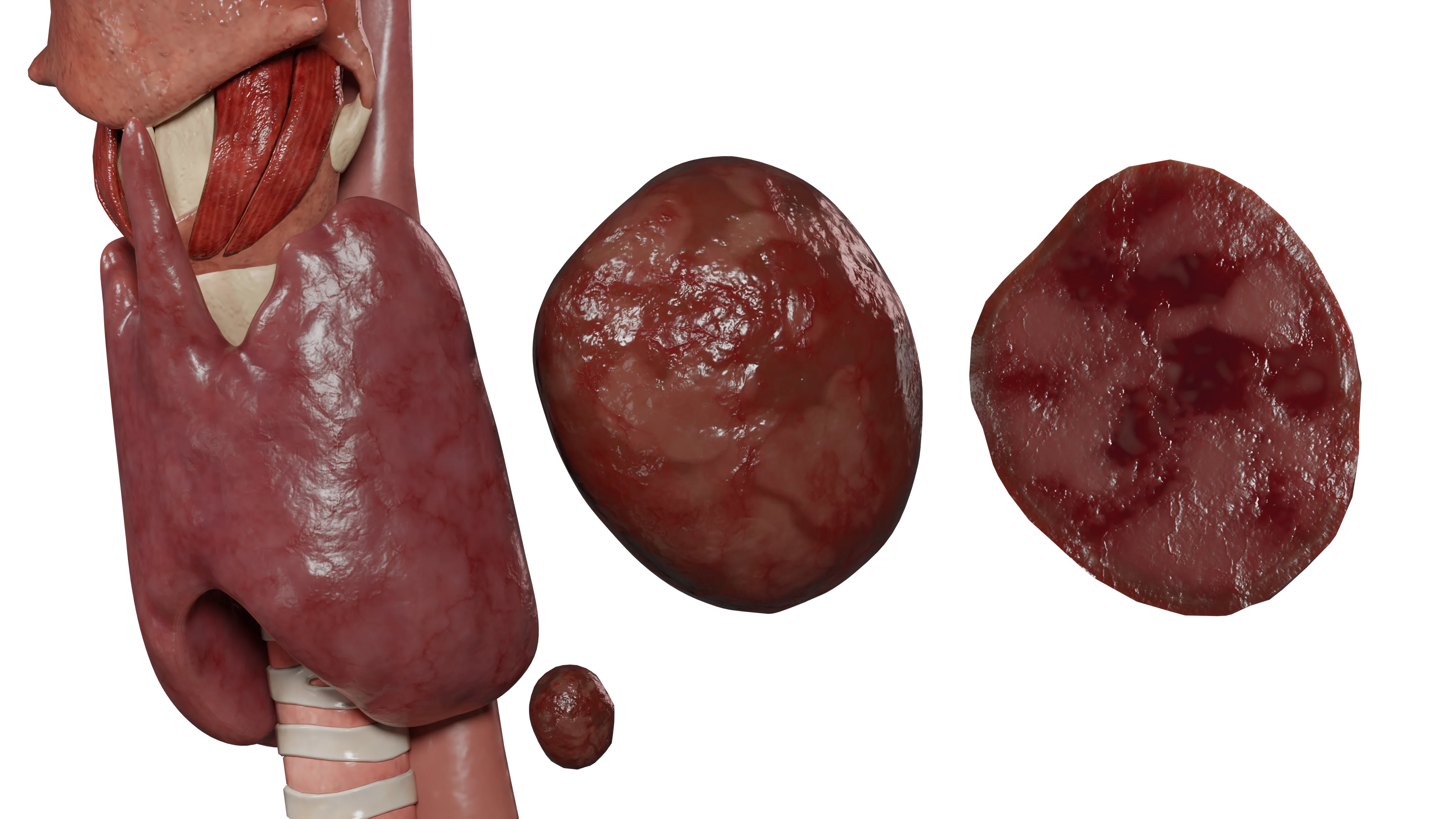
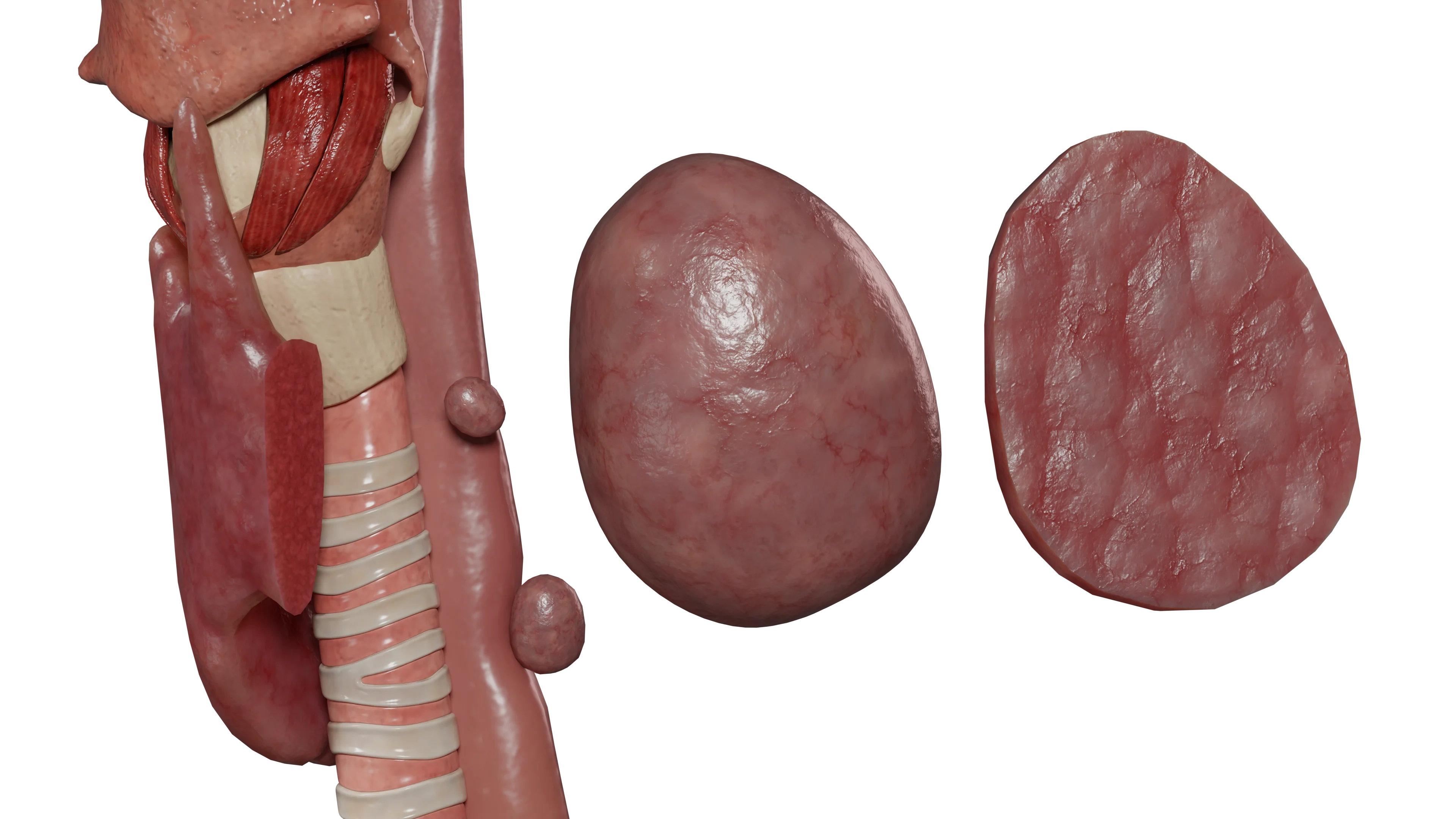
In the overwhelming majority of cases (80-85%), it is caused by an adenoma of one of the parathyroid glands. Less commonly, parathyroid gland hyperplasia and parathyroid gland carcinoma occur (less than 1%). It develops due to pathology of, most frequently, one of the parathyroid glands.
Parathyroid gland adenoma is characterized by the development of functional autonomy, leading to increased parathyroid hormone production.
Parathyroid gland adenoma can be sporadic or genetically determined (up to 10% of cases).
Parathyroid gland adenoma may occur in the following hereditary syndromes:
Multiple Endocrine Neoplasia (MEN) syndromes types 1, 2a, and 4;
Hyperparathyroidism-jaw tumor syndrome (HPT-JT);
Familial hypocalciuric hypercalcemia;
Familial isolated hyperparathyroidism.
Parathyroid hormone plays a crucial role in calcium-phosphate metabolism through the following mechanisms:
Enhancement of bone tissue resorption, resulting in the release of calcium and phosphorus into the blood serum;
Reduction of calcium excretion in the urine through increased renal reabsorption;
Activation of vitamin D 1-alpha hydroxylase, converting 25-hydroxyvitamin D to the active form (1,25-dihydroxyvitamin D), which increases calcium and phosphorus absorption in the gastrointestinal tract.
Furthermore, parathyroid hormone inhibits the reabsorption of phosphorus by the renal tubules, leading to hyperphosphaturia. This mechanism maintains serum phosphorus levels within or below the normal range.
In patients with primary hyperparathyroidism, the effect of increased calcium reabsorption may be offset by elevated hypercalcemia. In such cases, hypercalciuria will be detected.
Thus, patients with primary hyperparathyroidism are characterized by the following:
Increased levels of parathyroid hormone;
Hypercalcemia (due to bone tissue resorption and increased absorption of calcium and phosphorus in the gastrointestinal tract);
Normo- or hypophosphatemia;
Hyperphosphaturia;
Hypercalciuria with high serum calcium levels.
Secondary hyperparathyroidism: etiology and pathogenesis
Secondary hyperparathyroidism develops in the context of chronic kidney disease (CKD) as a compensation for prolonged hypocalcemia.
Its development involves the following mechanisms:
Renal dysfunction leads to a decrease in 1,25-dihydroxyvitamin D levels (activated from 25-hydroxyvitamin D in the proximal renal tubules), resulting in decreased calcium and phosphorus absorption in the gastrointestinal tract and the development of hypocalcemia;
Hypocalcemia stimulates calcium-sensitive receptors of the parathyroid glands, leading to increased production of parathyroid hormone;
Disorder of phosphorus excretion in CKD leads to hyperphosphatemia, directly activating the parathyroid glands and leading to increased parathyroid hormone production.
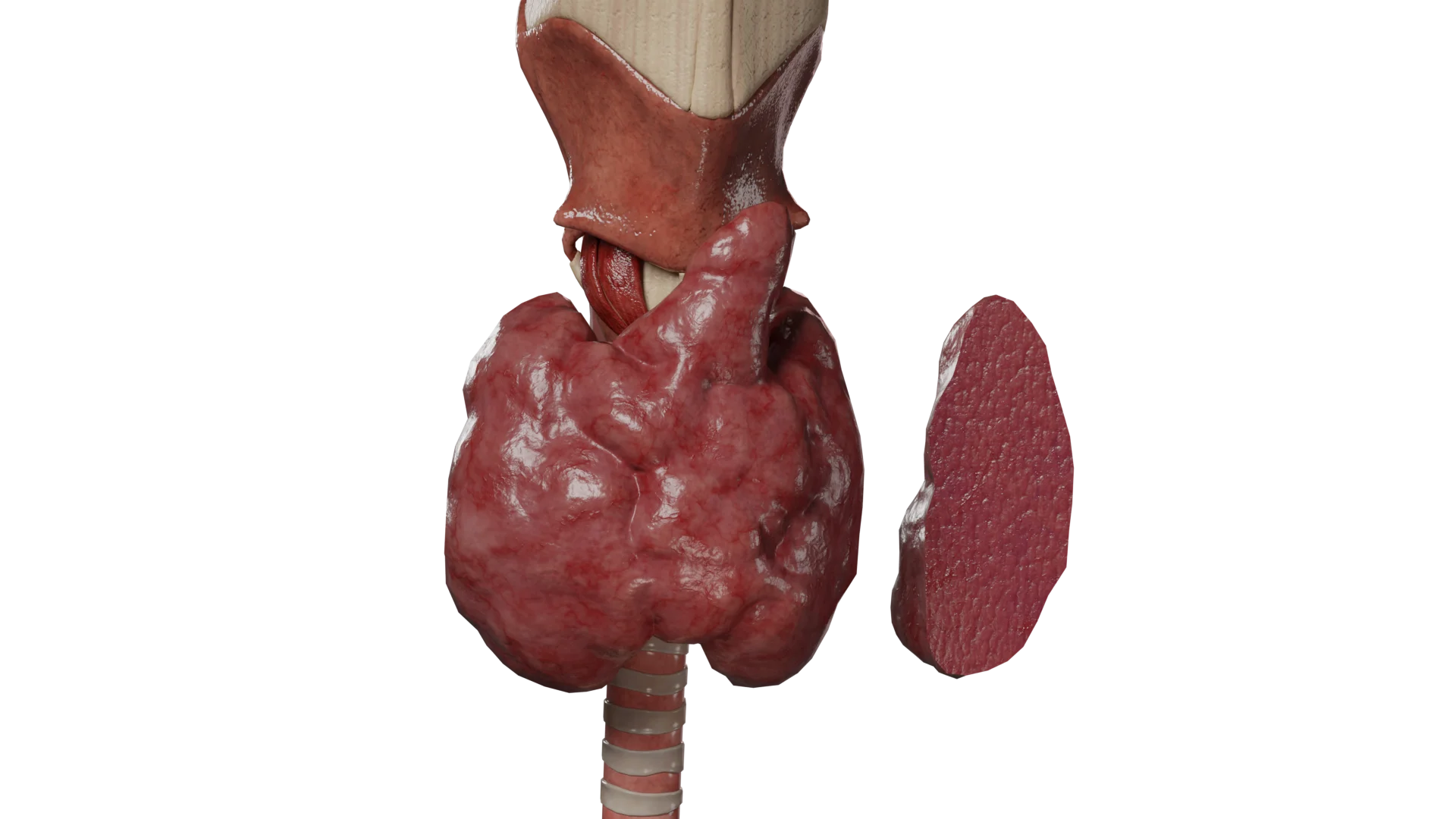
The aforementioned mechanisms result in continuous stimulation of the parathyroid glands’ function and, as a consequence, hyperplasia development.
Thus, secondary hyperparathyroidism is characterized by:
Increased levels of parathyroid hormone;
Hyperphosphatemia;
Hypocalcemia, rarely normocalcemia.
Tertiary hyperparathyroidism: etiology and pathogenesis
Tertiary hyperparathyroidism develops in association with long-term secondary hyperparathyroidism, leading to adenomatous transformation of the parathyroid glands with the development of functional autonomy.
Tertiary hyperparathyroidism is characterized by:
Significantly increased levels of parathyroid hormone;
Hypercalcemia;
Hyperphosphatemia;
Hyperphosphaturia and hypercalciuria.
Clinical presentation
Hyperparathyroidism can occur in three variants:
Subclinical or asymptomatic;
Manifest;
Acute, or hyperparathyroid crisis.
Currently, in the majority of cases, hyperparathyroidism is detected in the subclinical form through routine clinical and laboratory studies, and patients do not report any complaints at the time of diagnosis.
Manifest hyperparathyroidism
Early symptoms of hyperparathyroidism are nonspecific. These include:
Increased fatigue;
Muscle weakness;
Brittle nails, hair loss;
Periodic joint and muscle pain, especially after physical activity;
Emotional lability, memory impairment.
Long-standing hyperparathyroidism leads to the development of osteoporosis, the symptoms of which are:
Bone, joint, and muscle pain, which worsens with physical activity;
Bone fragility, leading to fractures even with everyday load (so-called pathological fractures), which heal very slowly, often with significant bony callus development, deformity of the broken bone, and formation of false joints;
Tooth enamel erosion, loosening and loss of teeth;
Muscle tension and cramps, especially at night;
Postural changes and height reduction due to more evident thoracic kyphosis.
In addition to osteoporosis manifestations, hyperparathyroidism is characterized by the following symptoms caused by prolonged hypercalcemia:
From the kidneys and urinary system:
Nephrolithiasis;
Polyuria;
Polydipsia.
Cardiovascular system:
Calcification of blood vessels and heart valves;
Hypertension;
Shortening of the QT interval, conduction disturbances leading to potentially life-threatening arrhythmias.
Gastrointestinal system:
Loss of appetite;
Nausea and vomiting;
Constipation;
Abdominal pain and flatulence;
Development of peptic ulcers of various localizations, prone to bleeding and recurrence.
A hyperparathyroid (or hypercalcemic) crisis is a life-threatening condition that develops in patients against a background of pre-existing hyperparathyroidism. Characterized by a rapid sharp increase in serum calcium levels above 3.5 mmol/L, with parathyroid hormone levels generally exceeding the norm by more than 20 times.
Provoking factors for crisis development may include infectious diseases, dehydration, and prolonged immobilization. Mortality ranges from 60 to 90% and requires immediate therapy in intensive care units.
Symptoms of hyperparathyroid crisis:
Severe vomiting, dehydration;
Abdominal pain;
Marked muscle weakness;
Lethargy, loss of consciousness, up to coma development.
Diagnosis
Main examination methods:
History and physical examination;
Laboratory diagnostics is the primary method for identifying hyperparathyroidism.
In a blood biochemistry, levels of parathyroid hormone, calcium (total and ionized), phosphorus, alkaline phosphatase (increased due to bone resorption), and vitamin D should be determined. Additionally, urinary calcium and phosphorus excretion levels are assessed (daily urine test).
Dynamic laboratory indicators for various variants of hyperparathyroidism:
Serum indicators
Primary hyperparathyroidism
Secondary hyperparathyroidism
Tertiary hyperparathyroidism
Parathyroid hormone
Elevated
Elevated
Significantly elevated
Calcium
Elevated
Normal or decreased
Elevated
Phosphorus
Normal or decreased
Elevated
Elevated
Alkaline phosphatase
Elevated
Elevated
Elevated
Vitamin D
Low
Low
Low
Imaging methods for parathyroid glands:
Ultrasound (main imaging method);
Scintigraphy of the parathyroid glands with Tc99m (allows visualization of the functional activity of the parathyroid glands);
Additional imaging methods may include computed tomography and magnetic resonance imaging of the neck and mediastinum.
Additional examination methods:
Densitometry to assess bone mineral density;
Ultrasound of the kidneys and urinary tract to identify nephrolithiasis;
Radiography of bones and joints.
Radiological signs characteristic of hyperparathyroidism:
Subperiosteal bone resorption;
Subchondral resorption;
Subenthesial resorption;
Intracortical resorption;
Acro-osteolysis;
Osteopenia;
Chondrocalcinosis;
Salt and pepper sign on skull radiograph;
Soft tissue calcification (in secondary and tertiary hyperparathyroidism);
Osteosclerosis.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of hyperparathyroidism
Primary hyperparathyroidism
The main treatment method is surgical. It enables the normalization of parathyroid hormone, calcium, and phosphorus levels in the shortest possible time, thereby reducing the risk of complications.
The operation involves the removal of the adenomatous altered parathyroid gland (parotidectomy), which is the gold standard for the therapy of primary hyperparathyroidism.
After the operation, the development of the “hungry bone” syndrome is possible, which is a persistent (more than 4 days) decrease in serum calcium levels. This syndrome is caused by a sharp decrease in parathyroid hormone levels after surgery, leading to increased osteoblastic activity and capture of calcium and phosphorus for bone tissue formation.
In a biochemical blood test, hypocalcemia, hypophosphatemia, hypomagnesemia, and elevated alkaline phosphatase levels are detected. This syndrome is more common in surgeries for secondary hyperparathyroidism.
Patients who have contraindications to surgical treatment may be assigned conservative therapy in cases of mild hypercalcemia and absence of complications. The following medications are used for the treatment of hyperparathyroidism:
Vitamin D. Dosage is selected individually to achieve the recommended level of 25-hydroxyvitamin D in the blood serum (30 ng/ml), which contributes to the reduction of bone tissue resorption.
Calcimimetics (cinacalcet, etelcalcitide). Significantly reduces parathyroid hormone and calcium levels in the blood serum but does not affect bone tissue resorption.
Denosumab (RANK ligand inhibitor). Inhibits bone tissue resorption. These drugs can be prescribed both alone and in combination for adequate control of parathyroid hormone, calcium, and bone mineral density levels.
In addition, patients receiving conservative therapy are not advised to restrict dietary calcium intake, as a deficiency in calcium intake may lead to stimulation of the parathyroid glands and an increase in parathyroid hormone levels.
Secondary and tertiary hyperparathyroidism
The main treatment method is conservative. Drug therapy is aimed at maintaining and, if possible, normalizing parathyroid hormone, calcium, and phosphorus levels.
In addition to the drugs used in primary hyperparathyroidism, vitamin D receptor activators are also used in the treatment of secondary and tertiary hyperparathyroidism:
Vitamin D metabolites (cholecalciferol, ergocalciferol);
Vitamin D analogues (calcitriol, paricalcitol, alfacalcidol, doxercalciferol).
If medical therapy is ineffective, surgical treatment is indicated. The extent of surgical intervention is determined individually, based on parathyroid hormone, calcium, phosphorus levels, the overall somatic state of the patient, and the presence of hyperparathyroidism complications.
The following operations can be performed:
Subtotal parathyroidectomy (leaving part of the parathyroid gland tissue). Minimal risk of permanent hypocalcemia, higher risk of recurrence.
Total parathyroidectomy without autotransplantation. Minimal risk of recurrence; the method has limitations due to the development of persistent hypocalcemia in the postoperative period, which is often poorly controlled with medications.
Total parathyroidectomy with autotransplantation of parathyroid gland tissue into the forearm muscles. The risk of recurrence is less than with subtotal parathyroidectomy, with a moderate risk of persistent hypocalcemia in the postoperative period.
Hyperparathyroid crisis
Treatment is conducted in an intensive care and resuscitation unit and includes the following:
Infusion therapy with large volumes of saline to replenish the circulating blood volume (rehydration);
Furosemide to force diuresis (calcium excretion);
Dialysis is possible, especially in patients with chronic renal failure;
Administration of bisphosphonates, calcimimetics, denosumab, calcitonin.
After stabilization of the condition, surgical treatment is indicated (parathyroidectomy for primary hyperparathyroidism and subtotal or total parathyroidectomy for secondary or tertiary hyperparathyroidism).
FAQ
1. What is hyperparathyroidism, and what are its consequences?
Hyperparathyroidism is an endocrine disorder associated with excessive secretion of parathyroid hormone (PTH). This leads to the leaching of calcium from bone tissue (resorption), causing osteoporosis and risk of fractures. An excess of calcium in the blood (hypercalcemia) contributes to the development of nephrolithiasis (kidney stones) and vascular and cardiac calcification.
2. What clinical symptoms of hyperparathyroidism are predominant in women?
The disease is diagnosed three times more often in women. The clinical presentation includes severe general weakness, bone and joint pain, and osteoporosis. Symptoms often present as non-specific, mimicking depression, memory impairment, or chronic fatigue syndrome.
3. What laboratory tests are necessary to verify the diagnosis?
Comprehensive laboratory diagnostics are conducted to confirm the diagnosis. Key serum indicators: level of parathyroid hormone (PTH), total and ionized calcium, phosphorus, alkaline phosphatase, and vitamin D. A daily urine analysis for calcium and phosphorus excretion is also required to assess mineral metabolism.
4. Is effective conservative therapy possible for primary hyperparathyroidism?
In primary hyperparathyroidism caused by an adenoma, the gold standard and only curative method remains surgical removal of the gland. Conservative therapy (bisphosphonates, calcimimetics) is used as a palliative measure when surgery is contraindicated or as a part of preparation for surgical intervention.
5. Why does secondary hyperparathyroidism develop in the context of kidney disease?
In chronic kidney disease (CKD), the synthesis of active vitamin D and phosphorus excretion is impaired, leading to a decrease in blood calcium levels. This triggers a compensatory mechanism: the parathyroid glands begin to work in an enhanced mode, which causes their hyperplasia and persistent elevation of parathyroid hormone levels over time.
6. What dietary therapy principles should be followed in hyperparathyroidism?
Patients are not advised to strictly restrict calcium in their diet, as its deficiency may further stimulate parathyroid hormone secretion. Monitoring of vitamin D levels is important. However, in secondary hyperparathyroidism caused by kidney pathology, it is critically important to limit foods high in phosphorus.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology
Available from: https://catalog.voka.io/
2.
Helbing A, Leslie SW, Levine SN. Primary Hyperparathyroidism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK441895/
3.
Muppidi V, Meegada SR, Rehman A. Secondary Hyperparathyroidism. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://www.ncbi.nlm.nih.gov/books/NBK557822/
4.
Palumbo VD, Damiano G, Messina M, Fazzotta S, Lo Monte G, Lo Monte AI. Tertiary Hyperparathyroidism: a review. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing.
Available from: https://pubmed.ncbi.nlm.nih.gov/33956045/
5.
Campos A. Hyperparathyroidism. PubMed [Internet].
Available from: https://radiopaedia.org/articles/hyperparathyroidism