Chemodectoma (Paraganglioma): Etiology, Pathogenesis, Classification, Diagnosis, and Treatment Methods
Oleg K.Cardiovascular surgeon, MD
10 min read·May 07, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
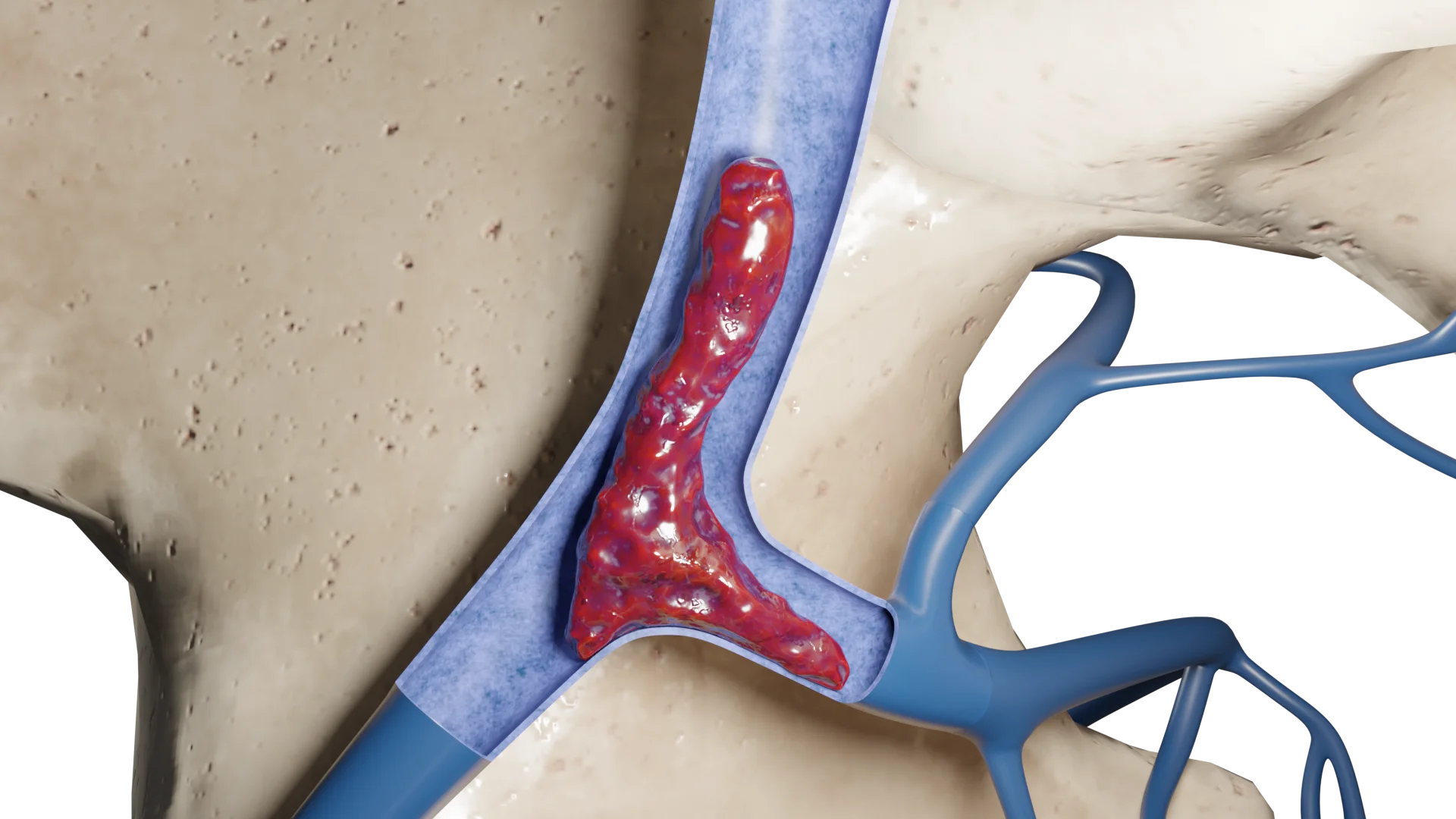
Carotid body paraganglioma (chemodectoma) is a rare, mostly benign tumor arising from the chemoreceptor cells of the carotid body located at the bifurcation of the common carotid artery.
Chemodectoma (paraganglioma)
Epidemiology
Approximately 1-2 cases per 100,000 population.
Women are affected more often than men.
The average age of diagnosis is about 45 years old.
The prevalence is high in Latin American countries, especially in Mexico, where women account for up to 90% of cases.
Residents of high altitude areas have an increased risk of developing chemodectomas due to chronic hypoxia.
Etiology
Genetic mutations: Mutations in genes encoding subunits of the succinate dehydrogenase complex (SDH), which is involved in the mitochondrial respiratory chain and cellular metabolism, play a leading role. Major genes:
SDHD is most commonly associated with multiple head and neck paragangliomas and is inherited paternally;
SDHB is associated with more aggressive forms and an increased risk of malignant progression;
SDHC, SDHA, SDHAF2 are less frequently involved but may also contribute to tumor development.
Syndromes associated with chemodectomas:
Von Hippel-Lindau syndrome (VHL);
Multiple endocrine neoplasia type 2 (MEN2);
Neurofibromatosis type 1 (NF1).
Chronic hypoxia: living at > 2000 m above sea level, as well as conditions such as chronic obstructive pulmonary disease and congenital heart disease, can stimulate carotid body hyperplasia.
Family history: about 10% of cases are familial.
3D animation – chemodectoma type I3D animation – chemodectoma type III
Pathogenesis
Hereditary mutations (SDHx)
Mutations of SDH (key enzyme of complex II of mitochondrial respiratory chain and Krebs cycle) → Accumulation of succinate (acts as “oncometabolite”) → Inactivation of prolyl hydroxylases (PHDs) enzymes, controlling degradation of HIF-1α (hypoxia-inducible factor) → Accumulation of HIF-1α → Pseudohypoxia → Activation of VEGF (angiogenesis)/ GLUT1 (glycolysis)/ PDGF (cell proliferation) → Neoplastic transformation of chemoreceptor cells and tumor formation.
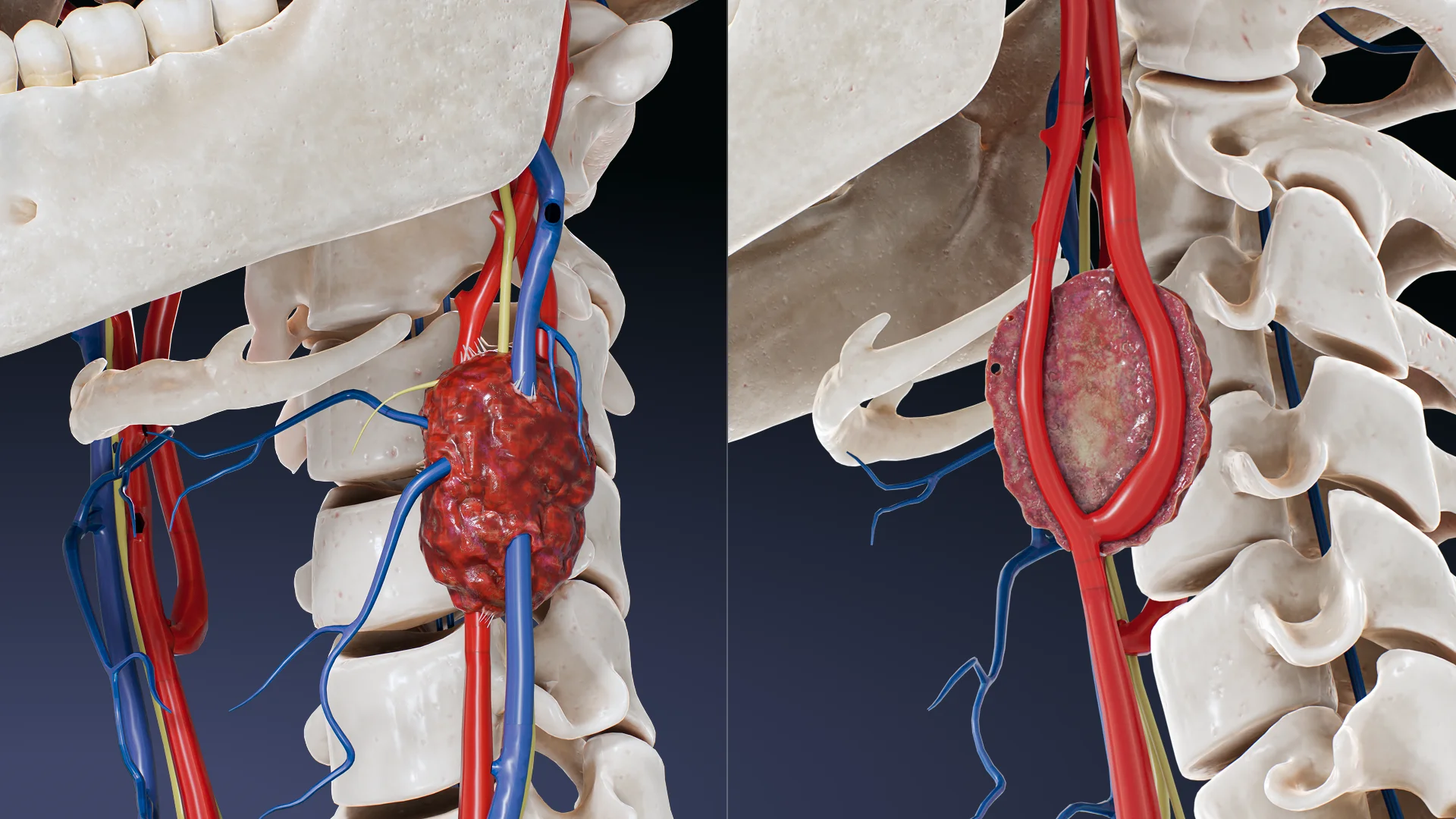
As a result, the tumor gradually increases in size. As it grows, it can demonstrate a locally invasive nature, to the point of encircling or compressing nearby anatomical structures – such as the internal and external carotid arteries, vagus, hyoid and lingual nerves – which can cause associated neurologic and vascular symptoms.
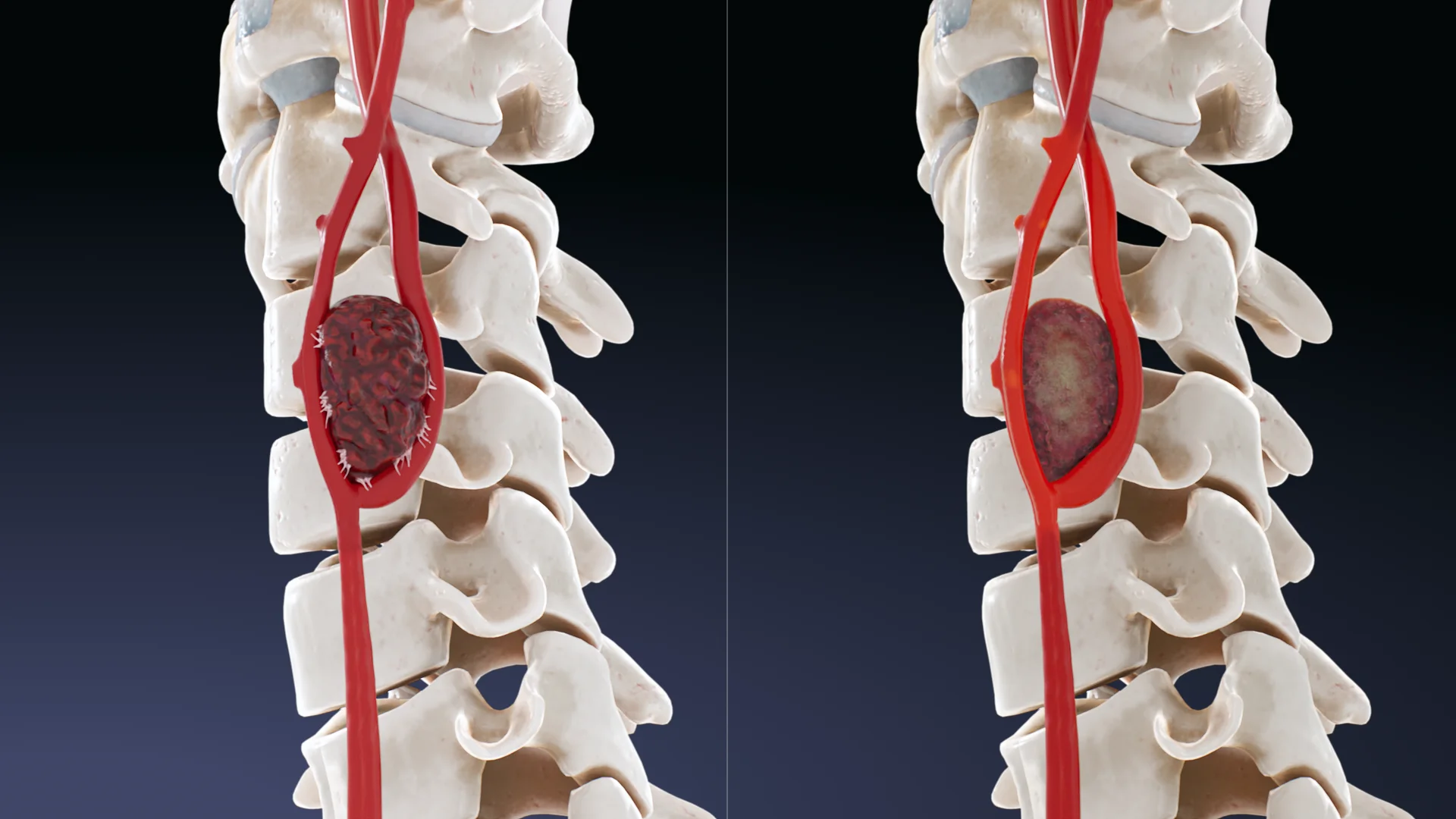
Classification of paraganglioma
W.R. Shamblin proposed to divide paragangliomas of the carotid calf into three types:
Type I: limited tumors up to 3.5 cm, loosely associated with arterial walls;
Type II: 3.5-5 cm, partially cover the carotid arteries, have a denser fusion with the arterial walls;
Type III: more than 5 cm, covering the carotid arteries and/or nearby vessels, nerves have a markedly dense fusion with these structures.
In addition, chemodectomas can be categorized by etiology: sporadic (up to 85%), familial (10-15%), and hyperplastic (1-5%).
For long periods of time, symptoms may be absent. As the tumor grows, complaints may appear:
Palpable tumor: slowly growing, painless, pulsating mass on the lateral surface of the neck (in the area of the sternoclavicular-papillary muscle);
Neurologic symptoms: hoarseness of voice, dysphagia, numbness of tongue caused by compression of cranial nerves (IX-XII);
Complaints related to catecholamine production (palpitations, attacks of arterial hypertension, sweating, headache, tremor);
Rarely: dizziness, fainting with carotid sinus compression.
Diagnosis of paraganglioma
Physical examination: dense, throbbing tumor on the neck, shifting horizontally but not vertically;
Ultrasound with Doppler: a hypervascular tumor in the region of the carotid bifurcation;
MRI with contrast: characteristic “salt-and-pepper” appearance on T1-weighted images;
CT with contrast: determination of the degree of invasion into vessels, evaluation of Shamblin classification. Construction of a 3D model for planning surgery;
Angiography: detection of the “lira sign” – divergence of the internal and external carotid arteries. Allows assessment of the need/ feasibility of embolization of the area as a step before surgical intervention;
PET-CT with 68Ga-DOTATATE: if multiple or metastatic foci are suspected;
Laboratory tests: plasma and urine levels of metanephrines and normetanephrines in suspected secreting tumor;
Genetic testing for mutations in SDH genes in the presence of family history or multiple tumors.
Treatment
Treatment of carotid chemodectoma depends on tumor size, clinical symptomatology, risk of complications, functional activity, genetic profile, and Shamblin grade. The main treatment modalities are surgical excision, preoperative embolization, and in some cases radiotherapy or chemotherapy.
Preoperative embolization
Preoperative embolization to reduce tumor vascularization and intraoperative blood loss, and to facilitate tumor isolation during surgery.
Indications:
Shamblin grade II-III tumors;
Tumor diameter >3 cm;
Presence of significant arterial blood flow (according to CT/angiography);
Planned resection with vascular reconstruction.
Contraindications:
Shamblin I tumors;
Absence of an arterial component (low vascularization);
Anastomoses with cerebral circulation – risk of cerebral embolization.
Methods: Selective angiography of the external carotid artery is performed. Embolizing agents are introduced through the microcatheter: polyvinylalcohol particles (PVA), microspheres, less commonly glue or spirals. Control angiography confirms blood flow reduction. Surgery is performed within 24-48 hours after embolization as long as the effect persists.
Find more scientifically accurate content on our social media
Extracapsular resection of the tumor. Standard for Shamblin I-II, vascular preservation, minimal risk;
Carotid resection with reconstruction. More often at Shamblin III. After resection of the carotid artery site, a prosthesis (Dacron, PTFE) is performed;
Neuromonitoring and microsurgery. It is used when close to cranial nerves (IX-XII).
Possible complications:
Bleeding (especially with inadequate embolization);
Damage to cranial nerves (IX-XII) – up to 30% in large tumors;
Stroke (when collateral blood flow is impaired);
Recurrence (rare, with incomplete resection).
Chemotherapy
It is not the standard treatment for carotid chemodectoma, as most tumors are slow growing and benign in nature. However, in rare cases of malignant course (rapid progression, metastatic lesions) or in inoperable metastatic forms, systemic therapy may be used.
Radionuclide therapy ¹⁷⁷Lu-DOTATATE (PRRT)
Prescribed in the presence of somatostatin receptor expression by PET with ⁶⁸⁸Ga-DOTATATE.
FAQ
1. Is carotid chemodectoma a malignant tumor?
In most cases, no. Carotid chemodectoma refers to benign, slow-growing tumors. However, in the presence of SDHB gene mutations, malignant potential with metastasis is possible.
2. Is it possible to just observe the carotid chemodectoma without removing it?
Yes, active surveillance is possible in some cases, especially if the tumor is small (<2.5 cm), asymptomatic, the patient is elderly, or there are contraindications to surgery. However, if there are signs of growth or compression of neck structures, treatment is required.
3 Is surgery to remove a carotid chemodectoma dangerous?
Risks depend on the size and location of the tumor. With large masses, complications including cranial nerve damage, bleeding, and ischemic events are possible. Preoperative embolization is often performed to reduce the risks.
4. Do other family members need to be screened if I am diagnosed with a chemodectoma?
If you are diagnosed with an inherited mutation (e.g., SDHD, SDHB), genetic counseling and screening of immediate family members is recommended, as the disease may be familial.
5. How can carotid chemodectoma be distinguished from other neck tumors?
Carotid chemodectoma is usually located at the bifurcation of the common carotid artery, is pulsatile, displaced horizontally but not vertically, and shows the characteristic “lyre sign” on CT/MRI. The diagnosis is clarified by imaging and angiography.
6. Can a chemodectoma cause pain or discomfort?
In most cases, no, especially in the early stages. However, as the tumor grows, it can cause pressure on nerves and blood vessels, resulting in pain, hoarseness of voice, trouble swallowing, or dizziness.
7. Is there a risk of recurrence after tumor removal?
If the tumor is completely removed, the risk of recurrence is low (less than 5%). However, with incomplete resection, hereditary form or presence of SDHB mutation, recurrence or development of new foci is possible. In such cases, long-term follow-up is important.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Luna-Ortiz, K., Reynoso-Noverón, N., Herrera-Ponzanelli, C., Favila-Lira, S., Luna-Peteuil, Z., Herrera-Gomez, A., & Gacia-Ortega, D. Y. Sex differences according to ethnic presentation in carotid body tumors: a systematic literature review. International Journal of Otorhinolaryngology and Head and Neck Surgery. 2022 Jun;8(6):527-531. DOI:10.18203/issn.2454-5929.ijohns20221393.
3.
Butt N, Baek WK, Lachkar S, Iwanaga J, Mian A, Blaak C, Shah S, Griessenauer C, Tubbs RS, Loukas M. The carotid body and associated tumors: an updated review with clinical/surgical significance. Br J Neurosurg. 2019 Oct;33(5):500-503. doi: 10.1080/02688697.2019.1617404.
4.
Darouassi Y, Alaoui M, Mliha Touati M, Al Maghraoui O, En-Nouali A, Bouaity B, Ammar H. Carotid Body Tumors: A Case Series and Review of the Literature. Ann Vasc Surg. 2017 Aug;43:265-271. doi: 10.1016/j.avsg.2017.03.167.
5.
Gonzalez-Urquijo M, Castro-Varela A, Barrios-Ruiz A, Hinojosa-Gonzalez DE, Salas AKG, Morales EA, González-González M, Fabiani MA. Current trends in carotid body tumors: Comprehensive review. Head Neck. 2022 Oct;44(10):2316-2332. doi: 10.1002/hed.27147.
6.
Ozawa H. Current management of carotid body tumors. Auris Nasus Larynx. 2024 Jun;51(3):501-506. doi: 10.1016/j.anl.2024.01.007.
7.
Piazza C, Lancini D, Tomasoni M, Zafereo M, Poorten VV, Hanna E, Mäkitie AA, Fernandez-Alvarez V, Kowalski LP, Chiesa-Estomba C, Ferlito A. Malignant carotid body tumors: What we know, what we do, and what we need to achieve. A systematic review of the literature. Head Neck. 2024 Mar;46(3):672-687. doi: 10.1002/hed.27624.

.webp)














/aortic%20dissection_main.webp)



