Vulvitis: Predisposing Factors, Clinical Manifestations, Diagnosis, and Treatment
Vulvitis refers to vulvar inflammation affecting the labia, clitoris, mons pubis, and vestibule of the vagina. Clinical manifestations, diagnosis, and treatment.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Genital herpesis a chronic viral infection that lasts for life. Two types of herpes simplex virus (HPV) can cause genital herpes: HPV-1 and HPV-2. Most cases of recurrent genital herpes are caused by HPV-2, with no detectable clinical manifestations, hence, in this case, genital herpes infection is transmitted by individuals who are not suspected of having the infection.
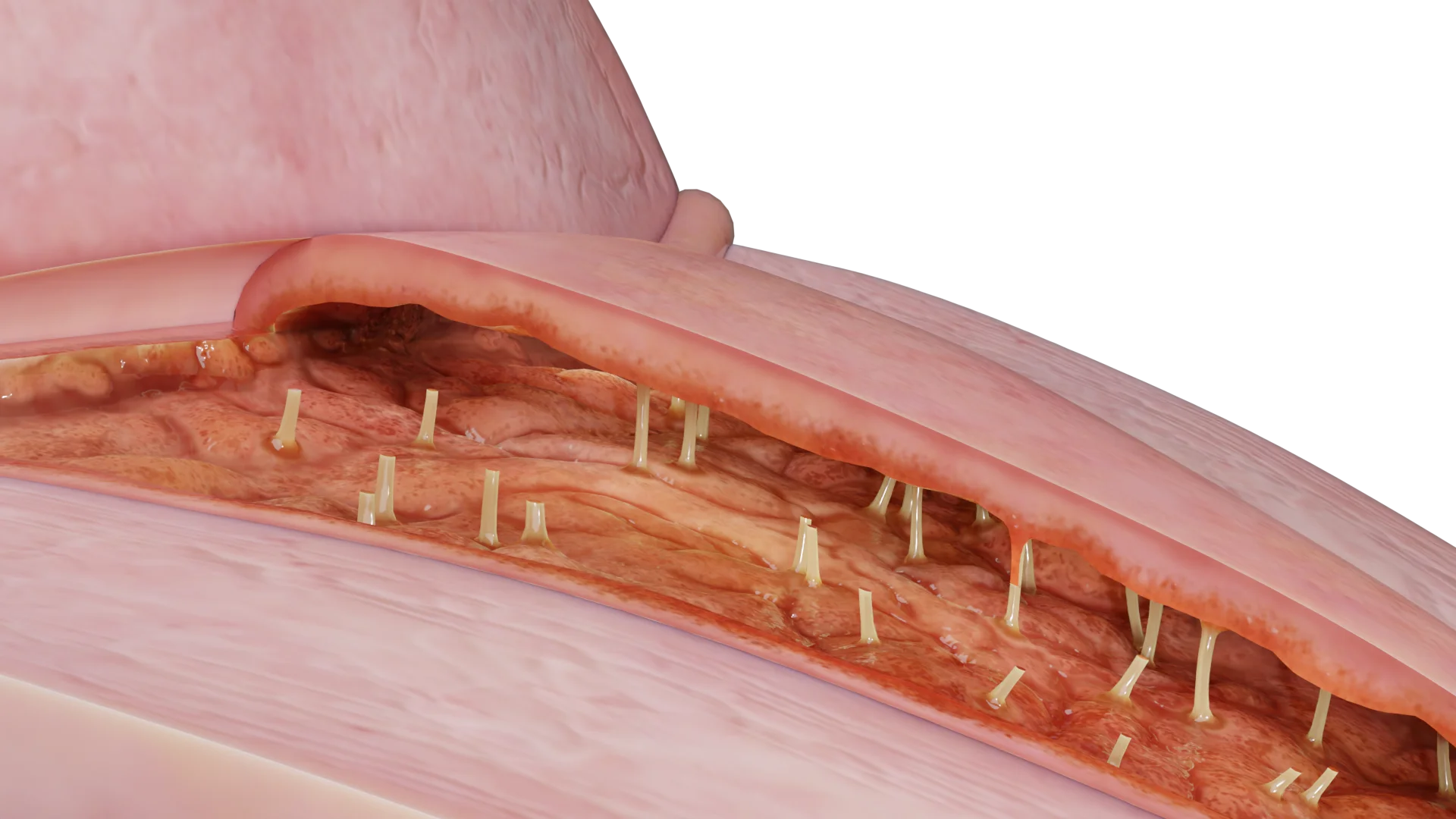
Herpetic vaginitis (vaginal herpes) during gynecologic examination in mirrors is manifested by swelling of the vaginal mucosa, painful vesicular rash or ulcerative lesions. The lesion process is usually self-limited.

When interviewed, the patient may mention complaints suggestive of neurologic symptoms. Non-specific symptoms may also be present: fever and enlarged lymph nodes, weakness.
The course of the disease can be completely asymptomatic.
Recurrent and subclinical courses are more common with infection caused by HPV-2. Vaginitis associated with HPV-2 increases the risk of HIV infection by two to three times, so all persons with genital herpes should be tested for HIV.
The difficulty in diagnosis is that self-limited, recurrent, painful, and vesicular or ulcerative lesions classically associated with HPV are absent in many infected individuals at the time of clinical evaluation.
All patients with a first episode of genital herpes should receive antiviral therapy. The standard course of treatment is 5-7 days. Treatment can be prolonged, if the therapeutic effect has not been achieved, up to 10 days of therapy.
Antiviral therapy may be instituted either in a suppressive drug regimen to reduce the frequency of recurrence or episodically to reduce or shorten the duration of lesions. Recurrences occur less frequently after the first episode of genital herpes HPV-1 compared with HPV-2. There are no data on the efficacy of suppressive therapy to prevent transmission of HPV-1.
All pregnant women should be interviewed for the presence of genital herpes or genital symptoms associated with HPV infection during pregnancy. Be sure to clarify the presence of prodromal symptoms (e.g., pain or burning at the site before vesicles appear). All women should be carefully screened for herpetic rashes to allow for vaginal delivery. Women with recurrent genital herpes should be delivered by cesarean section to reduce the risk of neonatal HPV infection, but the risk of transmission of HPV to the newborn is not eliminated. Treatment is recommended starting at 36 weeks of gestation. There are no data to support the use of antiviral therapy in HPV-seropositive asymptomatic women without a history of genital herpes.
Recommended treatment regimens for genital herpes
| Clinical situation | Recommended therapy regimens | Course duration | Notes |
|---|---|---|---|
| The first clinical episode | – Acyclovir 400 mg×3 p/d – Acyclovir 200 mg×5 p/d – Valacyclovir 1 g×2 p/d – Famciclovir 250 mg×3 p/d |
7-10 days | Start within the first 72 hours. If severe, extend to 10 days |
| Episodic therapy for relapses | – Acyclovir 800 mg×2 p/d – Valacyclovir 500 mg×2 p/d – Famciclovir 1 g×2 p/d (1 day) – Famciclovir 500 mg, then 250 mg×2 p/d |
3-5 days | Start in the prodromal period or in the first 24 hours of rashes |
| Suppressive therapy (frequent recurrences ≥6/year) ≥6/год) |
– Acyclovir 400 mg×2 p/d – Valacyclovir 500 mg×1 p/d – Valacyclovir 1 g×1 p/d – Famciclovir 250 mg×2 p/d |
Daily, long term | Reduces recurrences by 70-80%. For ≥10 recurrences/year – valacyclovir 500 mg/d may be less effective |
| Pregnancy (from week 36) |
– Acyclovir 400 mg×3 p/day – Valacyclovir 500 mg×2 p/day |
Before I gave birth | The goal is to reduce the risk of transmitting HPV to the newborn. Cesarean section for active rashes |
| HPV-1 (rare recurrences) |
Episodic therapy (similar to HPV-2) | 3-5 days | Suppressive therapy is not recommended because of the low recurrence rate |
Find more scientifically accurate content on our social media








The efficacy of male latex condoms has been established, which, when used consistently and correctly, can reduce but not eliminate the risk of genital herpes transmission. For patients with serologic evidence of HPV-2 (with combined testing if necessary) without symptomatic manifestations, neither episodic nor suppressive therapy is indicated for relapse prevention.
1. Can genital herpes be completely cured?
2. How is genital herpes transmitted?
3. What symptoms characterize the first episode of herpes?
4. Can genital herpes occur without symptoms?
5. How is the diagnosis of genital herpes confirmed?
List of Sources
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Workowski KA, Bachmann LH, Chan PA, Johnston CM, Muzny CA, Park I, Reno H, Zenilman JM, Bolan GA. Sexually Transmitted Infections Treatment Guidelines, 2021. MMWR Recomm Rep. 2021 Jul 23;70(4):1-187. PMID: 34292926.
3.
Watts DH, Brown ZA, Money D, et al. A double-blind, randomized,placebo-controlled trial of acyclovir in late pregnancy for the reduction of herpes simplex virus shedding and cesarean delivery. Am J Obstet Gynecol 2003;188:836–43. PMID:12634667.
4.
Scott LL, Hollier LM, McIntire D, Sanchez PJ, Jackson GL, Wendel GD Jr. Acyclovir suppression to prevent recurrent genital herpes at delivery. Infect Dis Obstet Gynecol 2002;10:71–7. PMID:12530483.
5.
Pinninti SG, Angara R, Feja KN, et al. Neonatal herpes disease following maternal antenatal antiviral suppressive therapy: a multicenter case series. J Pediatr 2012;161:134–8.e1-3. PMID:22336576.
6.
Leeyaphan C, Surawan TM, Chirachanakul P, et al. Clinical characteristics of hypertrophic herpes simplex genitalis and treatment outcomes of imiquimod: a retrospective observational study. Int J Infect Dis 2015;33:165–70. PMID:25660091.
7.
Wald A, Langenberg AG, Link K, et al. Effect of condoms on reducing the transmission of herpes simplex virus type 2 from men to women. JAMA 2001;285:3100–6. PMID:11427138.
8.
Aurelius E, Franzen-Röhl E, Glimåker M, et al.; HSV-2 Meningitis Study Group. Long-term valacyclovir suppressive treatment after herpes simplex virus type 2 meningitis: a double-blind, randomized controlled trial. Clin Infect Dis 2012;54:1304–13. PMID:22460966.
9.
Landry ML, Greenwold J, Vikram HR. Herpes simplex type-2 meningitis: presentation and lack of standardized therapy. Am J Med 2009;122:688–91. PMID:19559173.
10.
Wald A, Selke S, Warren T, et al. Comparative efficacy of famciclovir and valacyclovir for suppression of recurrent genital herpes and viral shedding. Sex Transm Dis 2006;33:529–33. PMID:16540883.
11.
Chosidow O, Drouault Y, Leconte-Veyriac F , et al. Famciclovir vs. aciclovir in immunocompetent patients with recurrent genital herpes infections: a parallel-groups, randomized, double-blind clinical trial. Br J Dermatol 2001;144:818–24. PMID:11298543.
12.
Leone PA, Trottier S, Miller JM. Valacyclovir for episodic treatment of genital herpes: a shorter 3-day treatment course compared with 5-day treatment. Clin Infect Dis 2002;34:958–62. PMID:11880962.
13.
Wald A, Carrell D, Remington M, Kexel E, Zeh J, Corey L. Two-day regimen of acyclovir for treatment of recurrent genital herpes simplex virus type 2 infection. Clin Infect Dis 2002;34:944–8. PMID:11880960.
14.
Bernstein DI, Bellamy AR, Hook EW 3rd, et al. Epidemiology, clinical presentation, and antibody response to primary infection with herpes simplex virus type 1 and type 2 in young women. Clin Infect Dis 2013;56:344–51. PMID:23087395.
15.
Van Der Pol B, Warren T, Taylor SN, et al. Type-specific identification of anogenital herpes simplex virus infections by use of a commercially available nucleic acid amplification test. J Clin Microbiol 2012;50:3466–3471. PMID:22875892.
16.
Binnicker MJ, Espy MJ, Duresko B, Irish C, Mandrekar J. Automated processing, extraction and detection of herpes simplex virus types 1 and 2: a comparative evaluation of three commercial platforms using clinical specimens. J Clin Virol 2017;89:30–3. PMID:2822627.
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io