Vulvitis: Predisposing Factors, Clinical Manifestations, Diagnosis, and Treatment
Vulvitis refers to vulvar inflammation affecting the labia, clitoris, mons pubis, and vestibule of the vagina. Clinical manifestations, diagnosis, and treatment.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Atrophic vaginitis is a complication of menopausal genitourinary syndrome, which is a constellation of signs and symptoms associated with a decrease in sex steroids, resulting in atrophic changes of the labia, clitoris, vaginal vestibule, vagina, vagina, urethra, and bladder.
Decreased levels of sex steroids, particularly estrogen, lead to atrophic changes in the vaginal mucosa and decreased glycogen deposition in the vaginal epithelium, which is metabolized by local bacterial communities to produce organic acids necessary for genital tract defense. As a result, the concentration of Lactobacillus is reduced and, as a consequence, the pH level rises, which stimulates the growth of pathogenic bacteria leading to vaginitis.
Androgens (i.e., dehydroepiandrosterone, androstenedione, and testosterone) play an important role in vaginal mucosal metabolism and are required for estrogen biosynthesis. In healthy premenopausal women, androgen production is significantly higher than estrogen production. Androgen receptors are widely distributed throughout the urogenital tract. Androgen-dependent protein products have trophic effects on various tissues of the urogenital organs (vaginal vestibule, clitoris, urethra, vagina, bladder, and pelvic floor muscles/ligaments). In addition to the cessation of estrogen production during menopause, the decrease in androgens with age may be a contributing factor to the signs and symptoms of genitourinary syndrome.
Patients are bothered by genital dryness, burning and irritation. Sexual symptoms such as lack of discharge, decreased lubrication, discomfort, pain during intercourse or vaginal bleeding associated with sexual activity. As well as symptoms of urinary dysfunction, dysuria and recurrent urinary tract infections. It is worth saying that these symptoms in postmenopause have a negative impact on sexual interest, intimacy and relationship with a partner, mood and self-esteem.
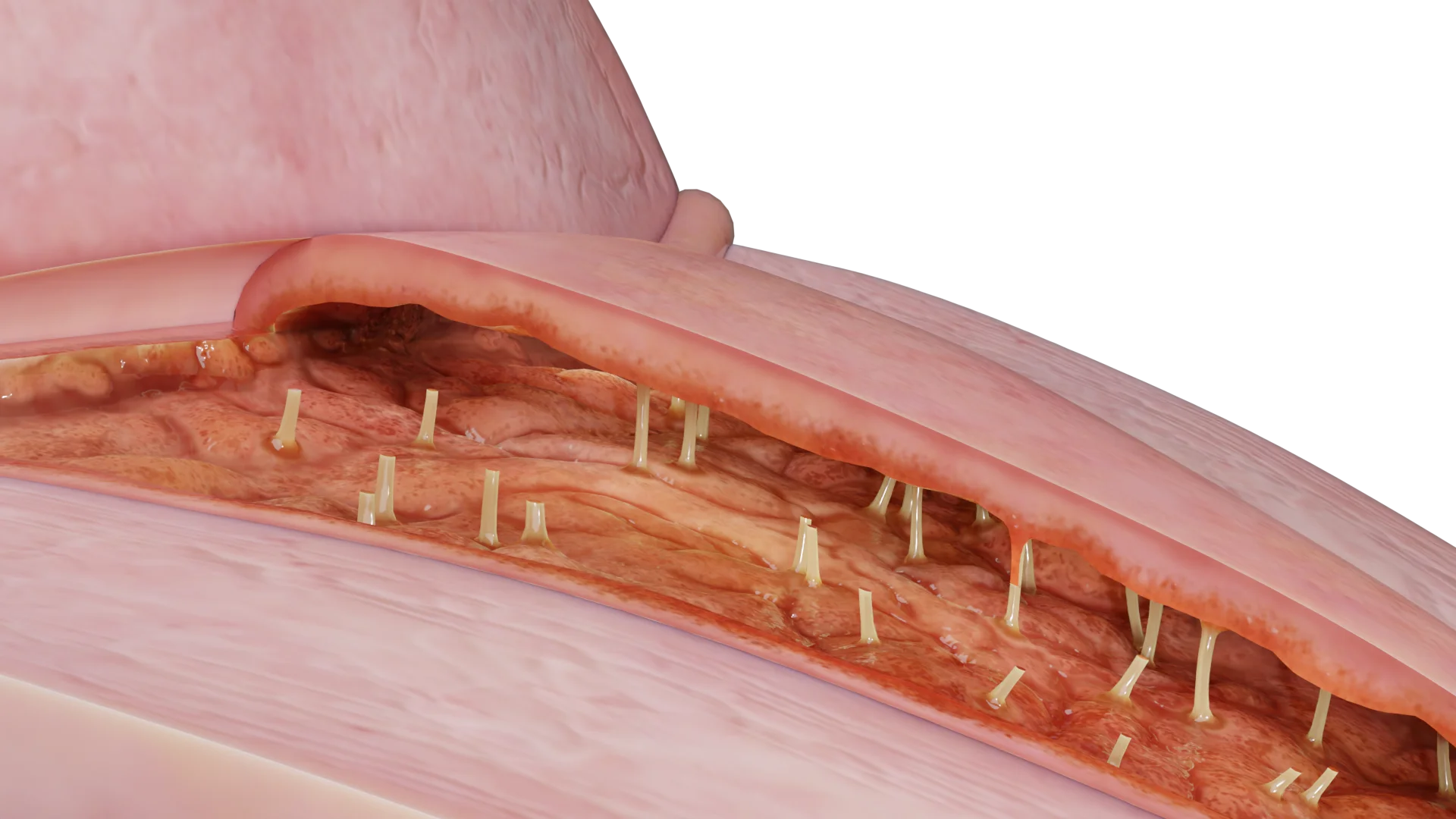
When examined in mirrors, thinning and smoothing of the vaginal mucosa, hyperemia, absence of discharge, the presence of local petechiae or ulcerative lesions are visualized.

The vaginal maturation index (VMI) is the proportional relationship between the superficial, intermediate, and parabasal cells of vaginal tissue. A decrease in estrogen is associated with an increase in parabasal cells, resulting in a decrease in VMI.
Histologic examination diagnoses a decrease in superficial squamous cells and an increase in parabasal cells. The hypoestrogenic state leads to loss of collagen, elastin fibers and blood vessels. These changes result in decreased elasticity and vascularization. Decreased vascularization in response to low estrogen levels leads to thinning of the vaginal mucosa and decreased discharge.
Vaginal therapy is the first-line pharmacologic treatment recommended by the International Menopause Society. Women should be started on the lowest dose and frequency that effectively manages their symptoms. The drug of choice is vaginal estrogen – this type of therapy is only appropriate for women with vaginal symptoms because this group of medications contains lower doses of estrogen than systemic therapy. Progestagen is generally not indicated for vaginal therapy. Endometrial surveillance is also not required unless there is postmenopausal bleeding that requires diagnostic evaluation. Vaginal therapy increases estrogen concentrations in the vaginal epithelium, uroepithelium, and helps reduce atrophic changes while minimizing systemic exposure. A Cochrane review showed no evidence of a difference in the proportion of women who reported improvement in symptoms between the following dosage forms: estrogen ring and estrogen cream, estrogen ring and estrogen tablets, estrogen tablets and estrogen cream. Estriol is a natural estrogen. A low dose of estriol vaginal gel (0.005%) has been shown to significantly increase vaginal cell maturation index and decrease vaginal pH compared to a control group in postmenopausal women.
Find more scientifically accurate content on our social media








1. Lubricants: women who do not wish to use vaginal estrogen can use non-hormonal lubricants and moisturizers. This therapy is aimed at short-term relief of vaginal dryness and dyspareunia. Water-based, silicone, mineral, or vegetable oil lubricants are applied to the vagina and vulva prior to intercourse.
2. Hyaluronic Acid:vaginal form of hyaluronic acid is a colorless gel that contains a derivative of hyaluronic acid that releases water molecules into the tissue, thereby relieving vaginal dryness without irritating the vaginal mucosa.
3. Physiotherapy/Dilators: Women with atrophic vaginitis and vaginal constriction can use a technique of gentle vaginal stretching using moistened dilators of various sizes. They will also be shown to perform exercises to train and relax the pelvic floor muscles.
4. Laser therapy: with fractionated CO2 laser or erbium:YAG laser. Several small studies have shown that fractional CO2 laser therapy can restore the vaginal epithelium to a premenopausal-like state, increase lactobacillus counts. However, the world’s leading experts have not endorsed fractionated CO2 laser therapy and caution against its use for the treatment of genitourinary syndrome without long-term well-controlled studies.
1. What is atrophic vaginitis?
2. What symptoms are characteristic of atrophic vaginitis?
3. What complications can develop if left untreated?
4. What preventive measures are recommended?
5. What age groups are characterized by atrophic vaginitis?
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Brotman R.M., Shardell M.D., Gajer P., Fadrosh D., Chang K., Silver M.I., Viscidi R.P., Burke A.E., Ravel J., Gravitt P.E.. Association between the vaginal microbiota, menopause status, and signs of vulvovaginal atrophy. Menopause. 2018 Nov;25(11):1321-1330.
3.
Cheng, R. Interpretation on the 2023 Chinese Menopause Symptom Management and Menopausal Hormone Therapy Guidelines. Med. J. Peking Union Med. Coll. Hosp. 2023, 14, 514–519.
4.
Partridge, L.; Deelen, J.; Slagboom, P.E. Facing up to the global challenges of ageing. Nature 2018, 561, 45–56.
5.
Valadares, A.L.R.; Kulak Junior, J.; Paiva, L.H.S.d.C.; Nasser, E.J.; da Silva, C.R.; Nahas, E.A.P.; Baccaro, L.F.C.; Rodrigues, M.A.H.; Albernaz, M.A.; Wender, M.C.O.; et al. Genitourinary Syndrome of Menopause. Rev. Bras. de Hematol. e Hemoter. 2022, 44, 319–324.




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io