Varicose Veins of the Lower Extremities: Etiology, Pathogenesis, Classification, Diagnosis, Treatment Methods
Oleg K.Cardiovascular surgeon, MD
12 min read·May 06, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
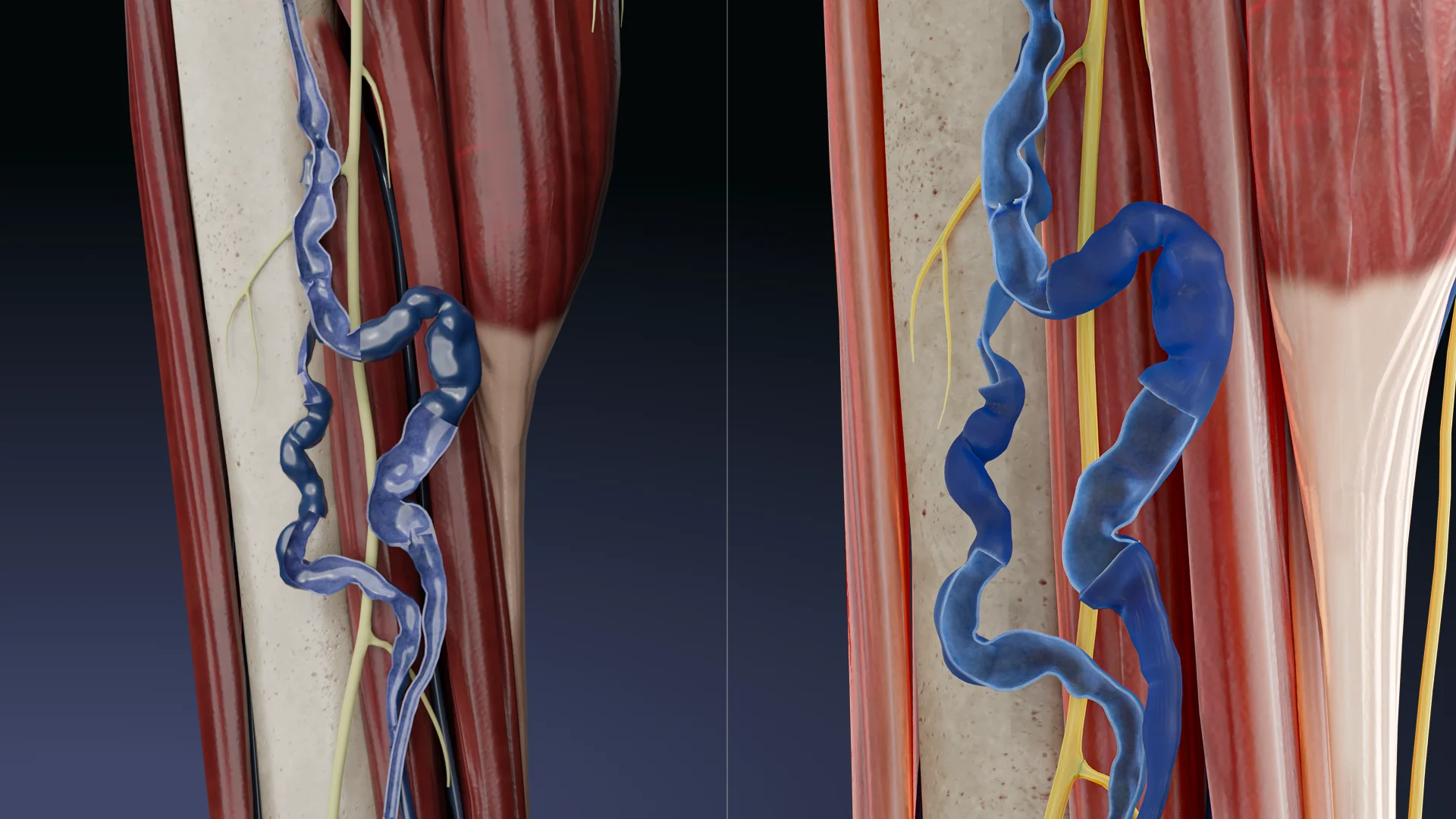
Varicose veins are a condition in which the vein wall becomes thin and the veins dilate unevenly.
Dilated, tortuous superficial veins (great and small saphenous veins) – 3D model
Epidemiology
Varicose veins of the lower extremities (VVLE) are among the most common chronic vascular diseases. According to epidemiological studies:
Prevalence in the adult population reaches 20–30%.
Women are affected 2–3 times more often than men, associated with hormonal influences and pregnancy.
The frequency increases with age: more than 50% of women and 30% of men over the age of 60 have signs of varicose veins.
Ethnic differences are minimal, but there is evidence of a slightly lower incidence in Afro-Caribbean populations compared to Caucasians.
Etiology
The development of varicose veins is caused by a combination of factors, the main ones being:
Heredity – genetic mutations affecting the structure of the venous wall and valves.
Female sex and hormonal changes – progesterone reduces venous wall tone.
Pregnancy – increased intra-abdominal pressure and hormonal effects.
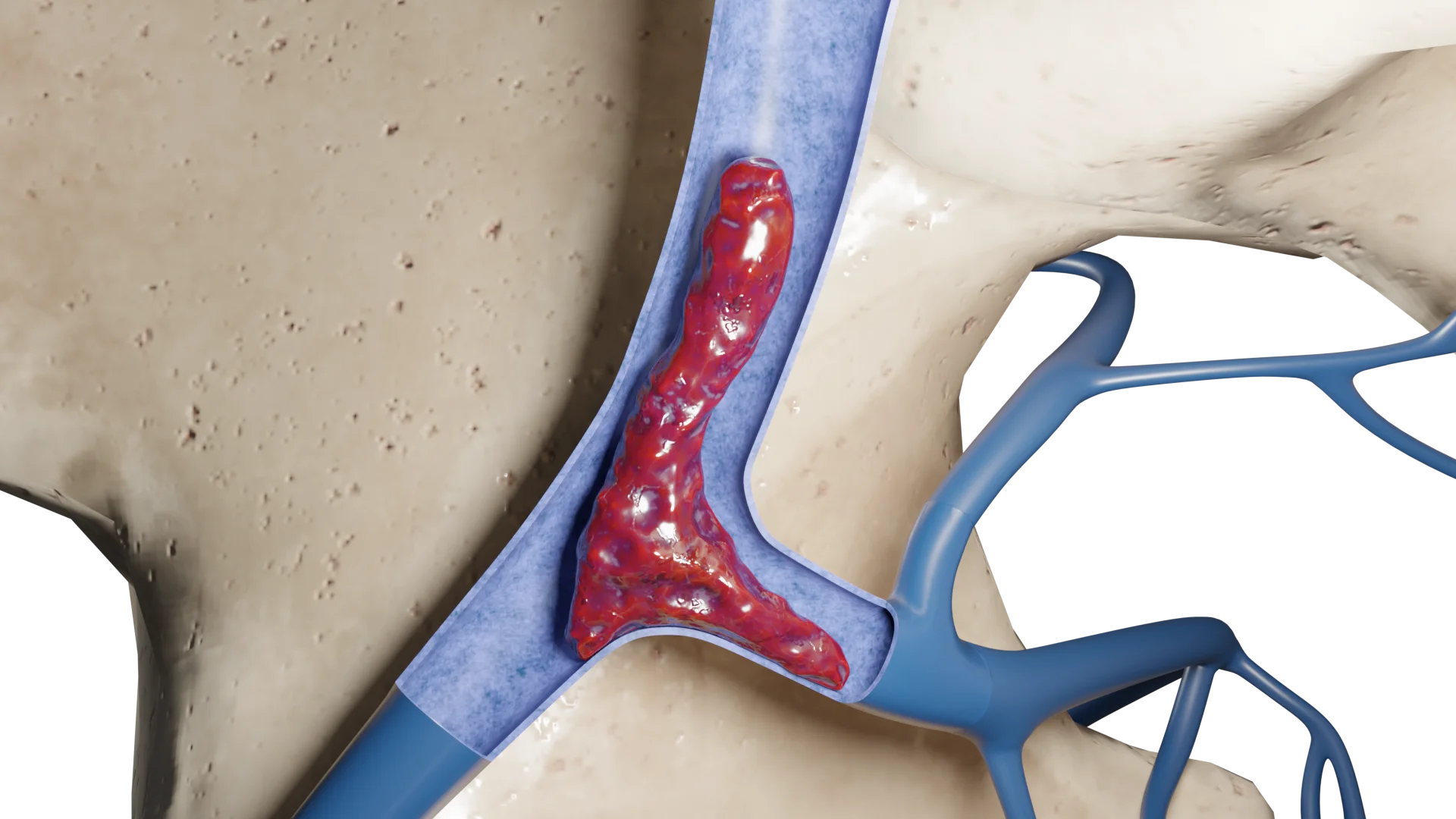
Venous hypertension leads to capillary stasis, hypoxia, and transendothelial leakage of plasma and erythrocytes. This causes edema, trophic skin changes, and, with progression, varicose ulcers, especially in the area of the medial malleolus, where hydrostatic resistance is the lowest.
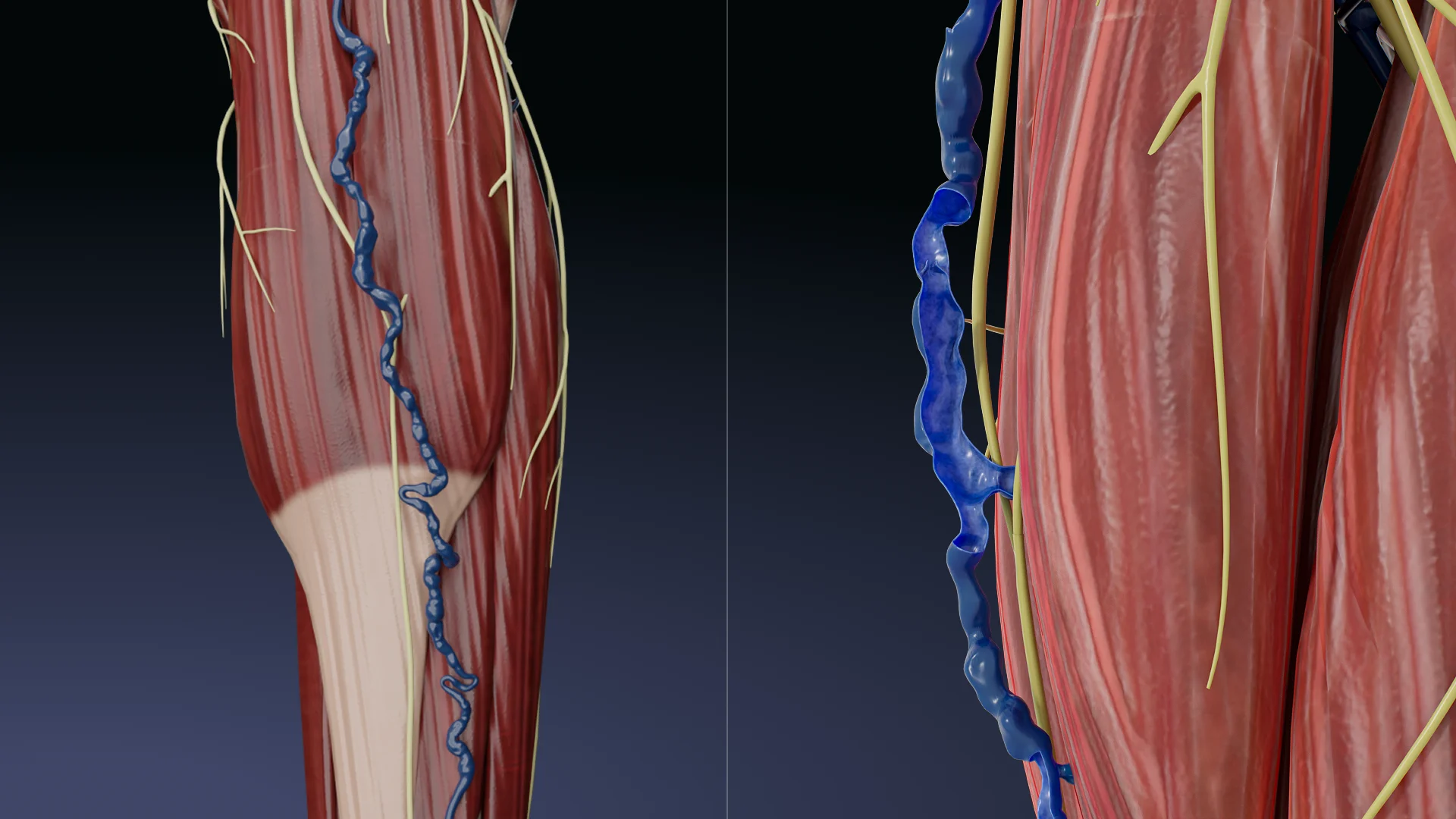
3D animation – development of varicosity of the small saphenous vein
Classification
The CEAP classification is used to assess the stage and severity of chronic venous disease: C – Clinical signs; E – Etiology; A – Anatomic location; P – Pathophysiologic mechanism.
C – Description
C0 – No visible or palpable signs of disease
C1 – Telangiectasias or reticular veins
C2 – Varicose veins (>3 mm in diameter)
C3 – Edema without skin changes
C4a – Pigmentation or eczema
C4b – Lipodermatosclerosis or white atrophy
C5 – Healed venous ulcer.
C6 – Active venous ulcer.
E – Value
Ec – Congenital
Ep – Acquired
Es – Secondary
En – Unspecified
A – Affected area
As – Superficial veins
Ap – Perforating veins
Ad – Deep veins
An – Unknown
R – Mechanism
Pr – Reflux (backflow of blood)
Po – Obstruction (e.g. thrombosis)
Pro – Reflux + Obstruction
Pn – Unknown
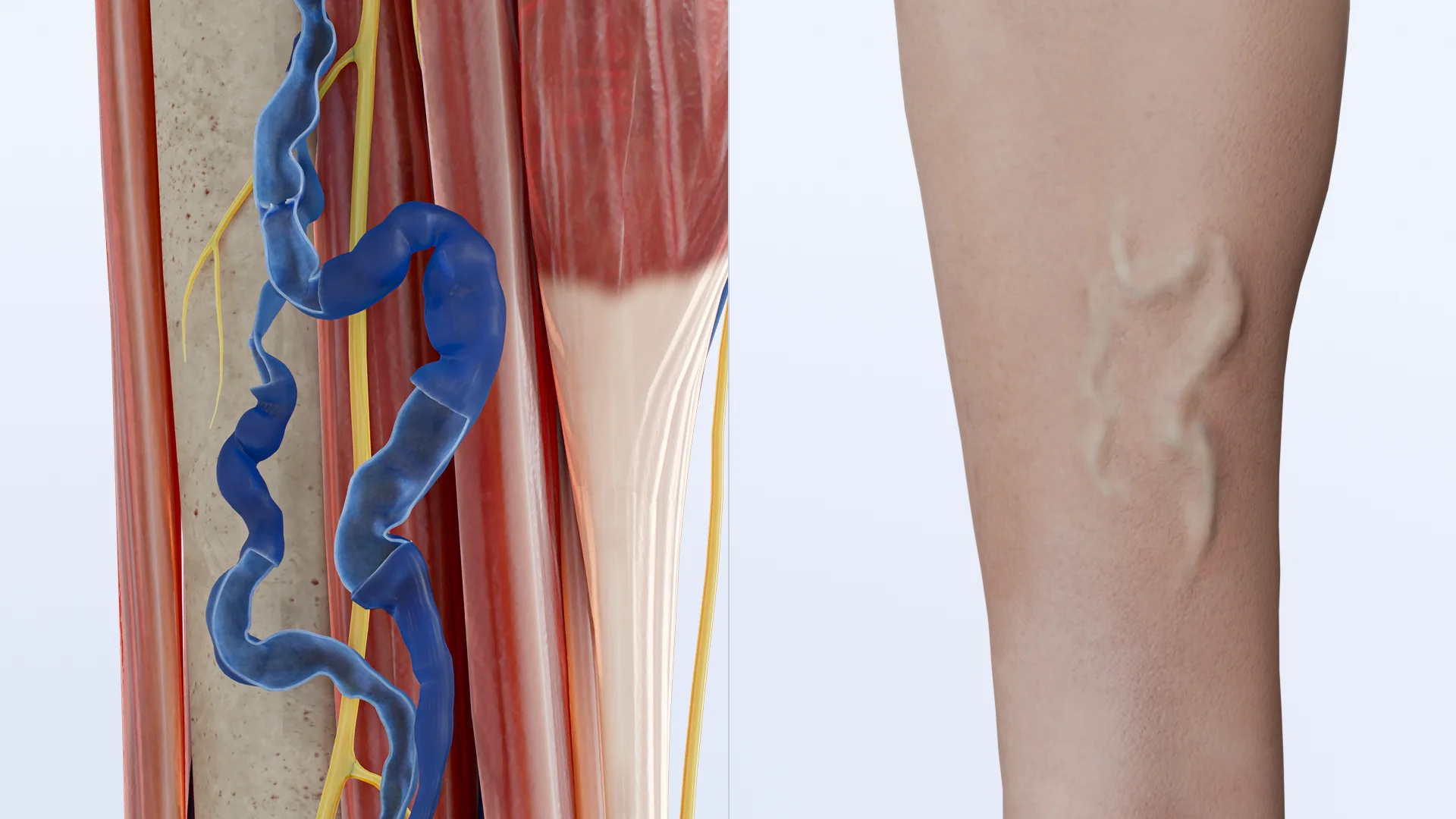
VV of the great saphenous vein – 3D modelVV of the small saphenous vein – 3D model
Clinical Manifestations
Symptoms range from cosmetic changes to severe trophic skin disorders:
Dilated, tortuous superficial veins.
Heaviness, fullness, and burning sensations in the legs.
Symptoms worsen with prolonged standing and improve with rest or leg elevation.
Diagnosis
Physical examination: Inspection and palpation of veins while standing.
Assessment of reflux (Trendelenburg test, Sheinis test).
Instrumental methods: Ultrasound angioscanning (duplex ultrasound) – the gold standard of diagnostics.
Imaging: Duplex ultrasound — the gold standard; reveals reflux, occlusions, vein diameter, and anatomy;
Pathologic reflux: >0.5 seconds post-compression.
Laboratory tests (in complications):
Coagulation panel — for suspected thrombosis.
Glucose, HbA1c — if diabetic angiopathy suspected.
Wound microbiota — if infected ulcers are present.
CEAP classification helps stratify risk and guide treatment decisions.
Treatment
1. Conservative Treatment
Compression therapy:
Elastic stockings come in different compression levels and are selected based on the stage of the disease and the severity of symptoms. An improperly selected garment may be ineffective or even harmful, so the type and class of compression should be prescribed by a doctor based on the examination.
They improve venous return, reduce edema, and alleviate subjective symptoms.
Venoactive drugs:
Diosmin, hesperidin, and troxerutin reduce capillary permeability and improve microcirculation.
They are used as symptomatic treatment, but do not address the underlying cause.
Lifestyle modifications:
Bodyweight management;
Moderate physical activity.
Avoiding prolonged sitting or standing
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
2. Surgical and Minimally Invasive Treatment
Indications:
Symptomatic varicose veins with confirmed reflux.
CEAP stages C2–C6.
Ineffectiveness of conservative therapy.
2.1. Endovenous laser ablation (EVLA)
Most common method.
Minimally invasive.
Laser causes thermal coagulation and vein sclerosis.
Performed under ultrasound and tumescent anesthesia.
2.2. Radiofrequency ablation (RFA)
Alternative to EVLA.
Uses radiofrequency energy.
Often better tolerated but more expensive.
2.3. Sclerotherapy
Injection of a sclerosing agent (foam or liquid) to close the vein.
Used for reticular veins and telangiectasias.
2.4. Miniphlebectomy (Müller technique)
Removal of varicose tributaries through micro-incisions.
2.5. Crossectomy and stripping
Resection of the great saphenous vein.
Used less often, when endovenous techniques are contraindicated.
Contraindications:
Acute thrombosis.
Decompensated chronic diseases.
Pregnancy (relative contraindication).
Active skin infections at the intervention site.
With timely and appropriate treatment, the prognosis is favorable. Modern endovenous techniques result in remission in 90–95% of cases. Recurrence is possible if technique is flawed or disease progresses.
Possible complications:
Thrombophlebitis.
Deep vein thrombosis (DVT).
Hyperpigmentation and hyperkeratosis.
Ulcerative and necrotic skin changes.
Bleeding from a varicose vein.
FAQ
1. Can varicose veins be treated without surgery?
It’s not possible to completely eliminate varicose veins without intervention, but conservative treatment (compression stockings, venotonics) can relieve symptoms and slow progression.
2. Which compression stockings are best, and can I choose them myself?
Stockings are selected based on compression class, disease stage, and anatomy. Self-selection may be ineffective or harmful — better to consult a doctor.
3. What are the risks of untreated varicose veins?
Without treatment, the condition can progress and lead to complications such as thrombophlebitis, swelling, hyperpigmentation, trophic ulcers, and even deep vein thrombosis.
4. Which surgical method is safest and most effective?
Endovenous laser coagulation (EVLC) and radiofrequency ablation (RFA) are considered the safest and most effective methods — minimally invasive, outpatient procedures with quick recovery.
5. Can I exercise with varicose veins?
Yes, but moderate dynamic activities like walking, swimming, and cycling are preferred. Heavy static loads and lifting weights without compression should be avoided.
6. Can varicose veins return after surgery?
Recurrence is possible, especially if there is a genetic predisposition or if recommendations after treatment are not followed, but modern methods provide long-lasting effects with the correct approach.
7. Is it necessary to treat varicose veins if there is no pain and only “spider veins”?
Telangiectasias and reticular veins are an early form of the disease. Although they often have cosmetic significance, it is important to undergo an examination to rule out hidden reflux.
8. Do varicose vein pills help?
Phlebotropic drugs help reduce swelling, heaviness, and cramps, but do not eliminate pathological reflux. They are used as part of combination therapy or when surgery is not possible.
List of Sources
1.
VOKA Catalog.
https://catalog.voka.io/
2.
Gloviczki P, Lawrence PF, Wasan SM, Meissner MH, Almeida J, Brown KR, Bush RL, Di Iorio M, Fish J, Fukaya E, Gloviczki ML, Hingorani A, Jayaraj A, Kolluri R, Murad MH, Obi AT, Ozsvath KJ, Singh MJ, Vayuvegula S, Welch HJ. The 2023 Society for Vascular Surgery, American Venous Forum, and American Vein and Lymphatic Society clinical practice guidelines for the management of varicose veins of the lower extremities. Part II: Endorsed by the Society of Interventional Radiology and the Society for Vascular Medicine. J Vasc Surg Venous Lymphat Disord. 2024 Jan;12(1):101670. doi:10.1016/j.jvsv.2023.08.011.
3.
Gloviczki P, Lawrence PF, Wasan SM, Meissner MH, Almeida J, Brown KR, Bush RL, Di Iorio M, Fish J, Fukaya E, Gloviczki ML, Hingorani A, Jayaraj A, Kolluri R, Murad MH, Obi AT, Ozsvath KJ, Singh MJ, Vayuvegula S, Welch HJ. The 2022 Society for Vascular Surgery, American Venous Forum, and American Vein and Lymphatic Society clinical practice guidelines for the management of varicose veins of the lower extremities. Part I. Duplex Scanning and Treatment of Superficial Truncal Reflux: Endorsed by the Society for Vascular Medicine and the International Union of Phlebology. J Vasc Surg Venous Lymphat Disord. 2023 Mar;11(2):231-261.e6. doi: 10.1016/j.jvsv.2022.09.004.
4.
Youn YJ, Lee J. Chronic venous insufficiency and varicose veins of the lower extremities. Korean J Intern Med. 2019 Mar;34(2):269-283. doi: 10.3904/kjim.2018.230.
5.
Gwozdzinski L, Pieniazek A, Gwozdzinski K. Factors Influencing Venous Remodeling in the Development of Varicose Veins of the Lower Limbs. Int J Mol Sci. 2024 Jan 26;25(3):1560. doi: 10.3390/ijms25031560.
6.
Chung JH, Heo S. Varicose Veins and the Diagnosis of Chronic Venous Disease in the Lower Extremities. J Chest Surg. 2024 Mar 5;57(2):109-119. doi: 10.5090/jcs.23.110.
7.
Adler C, Mousa A, Rhee A, Patel MD. Varicose Veins of the Lower Extremity: Doppler US Evaluation Protocols, Patterns, and Pitfalls. Radiographics. 2022 Nov-Dec;42(7):2184-2200. doi: 10.1148/rg.220057.
8.
Gawas M, Bains A, Janghu S, Kamat P, Chawla P. A Comprehensive Review on Varicose Veins: Preventive Measures and Different Treatments. J Am Nutr Assoc. 2022 Jul;41(5):499-510. doi: 10.1080/07315724.2021.1909510.















.webp)
/aortic%20dissection_main.webp)



