Hydronephrosis: Clinical Presentation, Symptoms, Diagnostics, and Treatment

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
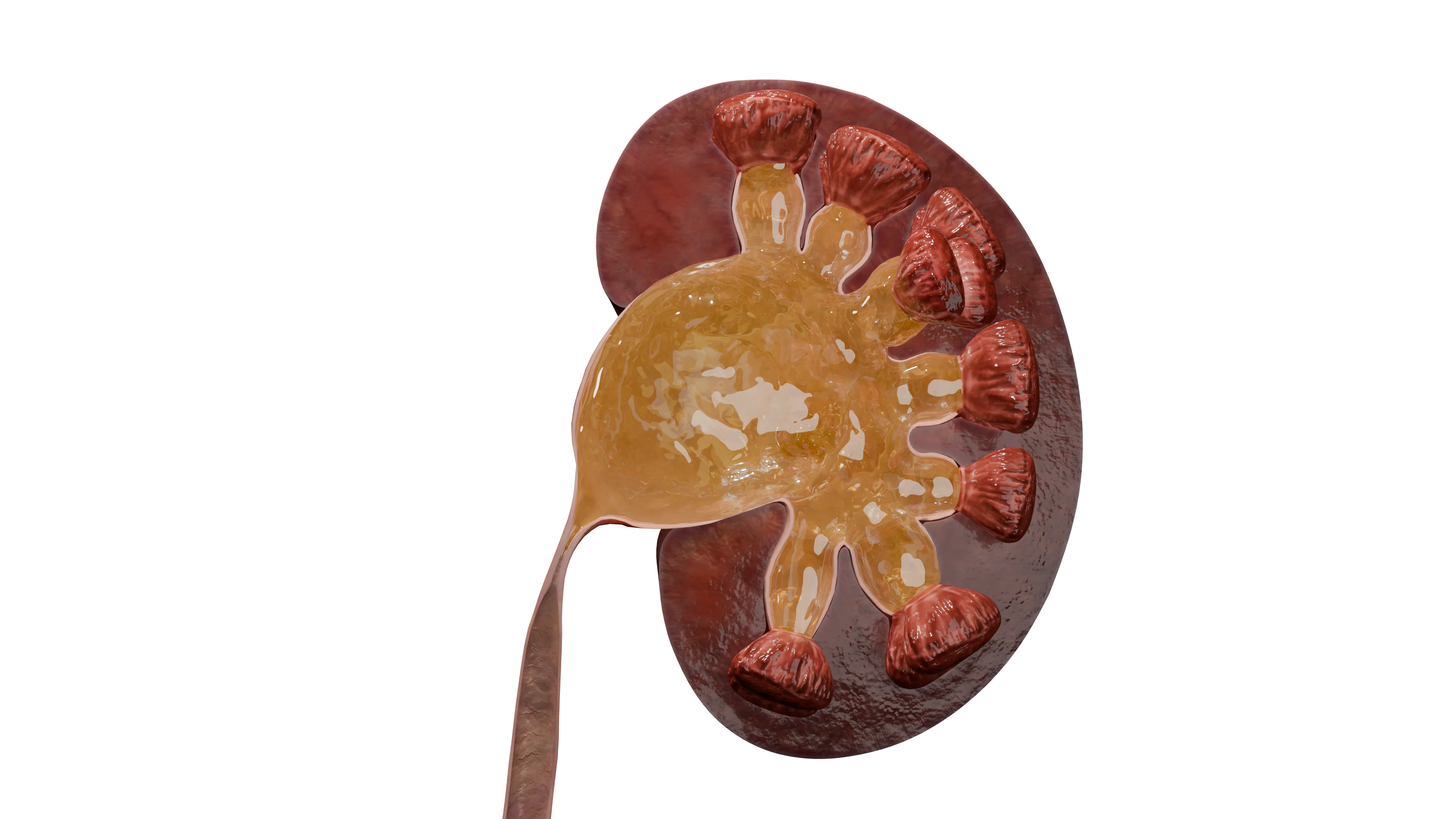
Hydronephrosis is a pathological condition characterized by progressive dilation of the renal collecting system. This dilation occurs due to an obstruction at any level of the urinary tract, leading to an impairment of normal urine flow. Prolonged elevation of intrarenal pressure causes structural changes in the renal parenchyma, which, if not corrected in a timely manner, can lead to irreversible organ dysfunction.

Modern classifications of hydronephrosis focus on three key aspects: etiology, obstruction severity, and stage of parenchymal damage. By origin, there are congenital forms associated with abnormalities in the development of the urinary system and acquired forms caused by urolithiasis, tumors, or iatrogenic factors. The obstruction severity is assessed by uroflowmetric studies and determines the management strategy for the patient.
Incidence
The incidence of hydronephrosis shows significant geographical variations, ranging from 1:750 to 1:1,500 of live births. The sex ratio for incidence is 2:1, favoring males. Adult incidence is not clearly defined.
Etiology
Congenital abnormalities of the urinary tract play a significant role in the etiology of hydronephrosis. Ureteropelvic junction stricture is the most common congenital cause of obstruction leading to progressive dilation of the renal pelvis.
Acquired forms of hydronephrosis develop as a result of various pathological processes impairing urine flow. Urolithiasis causes ureteric obstruction by calculi, resulting in acute dilation of the renal cavitary system. Tumors in the pelvis and retroperitoneal space can cause extraureteral compression, while ureteral strictures often develop after radiation therapy or surgery. Neurogenic bladder dysfunctions, including detrusor sphincter dyssynergia, lead to functional obstruction of the lower urinary tract.
Pathogenesis
Obstruction of the urinary tract is the primary factor in the development of hydronephrosis, creating a mechanical barrier to normal urine flow.
Impaired urine flow leads to progressive dilation of the renal collecting system, followed by an increase in intrapelvic pressure.
In response, hypertrophy of the muscle fibers of the pelvis and calyces occurs with enhanced peristalsis to overcome the obstructions. Constantly increased pressure has the following sequela:
- Atrophy of the renal parenchyma (compression of tubules and vessels, ischemia, death of nephrons with replacement by fibrous tissue);
- Impairment of renal blood flow (activation of the renin-angiotensin-aldosterone system, which can lead to renovascular hypertension);
- Urine flow disorder (retention of urine increases the risk of infection (pyelonephritis) and nephrolithiasis).
Clinical presentation
Clinical manifestations of hydronephrosis vary widely depending on the severity of the urinary tract obstruction and the duration of the pathological process.
In cases of acute complete obstruction, severe pain similar to renal colic is observed. In cases of partial or chronic obstruction, symptoms may be masked or completely absent due to the activation of compensatory mechanisms. The prolonged course of the disease leads to gradual atrophy of the renal parenchyma with a corresponding decrease in the functional activity of the organ.
Diagnosis of hydronephrosis
Ultrasound
Ultrasound examination (US) is the method of choice for the initial diagnosis of hydronephrosis due to its non-invasiveness, safety, and accessibility.
The main advantage of this method is the ability to visualize the dilation of the renal collecting system without using ionizing radiation, which is especially important for pregnant women and children. The technology allows for dynamic monitoring of changes in the renal parenchyma and the degree of dilation of the renal cavitary system.
Radiological methods
Excretory urography and multislice computed tomography (MSCT) with contrast enhancement are key methods for assessing the grade of obstruction of the urinary tract in hydronephrosis patients. These techniques allow visualization of the renal cavitary system anatomy and determine the level and extent of ureteral narrowing. Retrograde pyeloureterography is used when excretory studies don’t provide enough comprehensive information about the distal portions of the urinary tract. These methods are invaluable for planning surgery.
In cases of chronic hydronephrosis, X-ray contrast studies show distinctive morphofunctional changes in the renal parenchyma. Thinning of the cortical layer, reduction in parenchymal thickness, and deformation of the renal collecting system reflect the degree of chronic injury. Decline in excretory function at late stages manifests with delayed excretion of the contrast agent.
Dynamic diuretic renal scintigraphy is a radioisotope method that assesses kidney function and urinary tract patency. Its main idea is that a diuretic (furosemide) is injected intravenously to create a “hydraulic load” following the administration of the radiopharmaceutical and its accumulation in the pelvis. The rate of the radiopharmaceutical elimination from the dilated pelvis determines whether a mechanical obstruction is present or outflow is adequate.
Quantitative parameters assessed in dynamic nephroscintigraphy:
- Separate function of the kidneys. The normal range is 45-55% for each kidney. It may decrease with obstruction.
- Time to peak activity (Tmax). Normal values range from 3 to 5 minutes. They increase with obstruction.
- Half-life (T½) after diuretics:
- T½ < 10 minutes indicates no obstruction.
- T½ = 10-20 minutes is a borderline result.
- T½ > 20 minutes indicates obstruction.
The higher the value, the greater the obstruction.
Static nephroscintigraphy is a radionuclide diagnostic method that involves imaging and assessing the anatomical and functional state of the renal parenchyma (functioning tissue) rather than the process of urine excretion. The method shows the distribution of the functioning tissue, detects areas of damage (scars, ischemic zones), and allows precise determination of each kidney function separately, which is critically important for deciding on organ preservation in severe hydronephrosis.
Find more scientifically accurate content on our social media








Treatment
The goal of hydronephrosis treatment is to eliminate obstruction, restore urine flow, preserve kidney function, and prevent complications. The choice of method depends on the degree of hydronephrosis, kidney function, length and cause of the stricture, as well as the surgeon’s experience.
The main principle of surgical treatment is the reconstruction of the ureteropelvic junction (ureteropyeloplasty). In cases of severe hydronephrosis with more than 90% loss of function, nephrectomy (removal of the kidney) is indicated.
Main types of reconstructive surgeries:
- Anderson-Hynes open ureteropyeloplasty. It involves excising the narrowed UPJ segment and re-anastomosing it to the renal pelvis to create a wide drainage pathway.
- Laparoscopic ureteropyeloplasty. A minimally invasive alternative to open surgery with similar long-term results.
- Robot-assisted ureteropyeloplasty.
- Endoscopic (endoureteral) methods. They are used for short strictures (less than 1-2 cm), especially postoperative, or in patients with high surgical risk.
- Dilation (including balloon dilation). It refers to the mechanical dilation of the structure. The effectiveness is low, whereas the risk of recurrence is high.
- Endoureterotomy (using a cold knife or a laser). It’s a longitudinal dissection of the structure (either retrograde or antegrade) under visual control.
Alternative and auxiliary methods
- Kidney autotransplantation. It is used for extensive strictures of the entire ureter in cases where reconstruction is not possible.
- Percutaneous nephrostomy. Can be chosen as a palliative method for inoperable patients or for temporary urine drainage prior to definitive surgery.
- Placement of a permanent internal stent into the ureter. Applicable for patients with high surgical risk.
FAQ
1. What is hydronephrosis, and how does this condition progress?
2. What are the risks to the patient if timely treatment is not provided?
3. Can hydronephrosis resolve on its own?
4. Which study allows for the most accurate assessment of kidney function in hydronephrosis?
5. What is the advantage of Anderson-Hynes pyeloplasty over other methods?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Gafurov AA, Ibragimov ZhKh. [Analysis of long-term results of surgical treatment of hydronephrosis in children]. Journal of modern medicine. 2024;(4):583-587. [In Russian.]
3.
Gafurov AA, Ibragimov ZhKh. [Analysis of long-term results of surgical treatment of hydronephrosis in children]. Journal of modern medicine. 2024;(4):583-587. [In Russian.]
4.
Ivanova IE, Rodionov VA, Semenova LV. [Chronic kidney disease in children of the Chuvash Republic]. Pediatriia. 2011;(3):138-142. [In Russian.]
5.
Mavlyanov FSh, Mavlyanov ShKh. [Results of surgical treatment of obstructive uropathies in children depending on the level and degree of obstruction]. Voprosy meditsiny. 2022:98-107. [In Russian.]
6.
Suvorova AV, Zenchenko OA. [Possibilities of laboratory diagnostics and monitoring in neonatal nephrology]. In: Aktual’nye voprosy pediatrii i gemostaziologii. Novosibirsk; 2008. p. 179-183. 179-183. [In Russian.]
7.
Chernetsova GS, Kolesnichenko IV, Chernetsov ON. [Main issues of surgical correction of hydronephrosis in various age groups]. Bishkek: KRSU; 2014. 91 p. [In Russian.]
8.
Shirov TF, Mardieva GM, Rustamov UKh. [Radiological research methods in the diagnosis of hydronephrosis]. Problemy biologii i meditsiny. 2015;(2):192-195. [In Russian.]
9.
Shukurov IA, Chernetsova GS, Teifurov DS, et al. [Drug treatment of acute and chronic kidney diseases in obstructive uropathies (literature review)]. Voprosy urologii. 2023;(3):168-172. [In Russian.]




Loading test 6 questions



