Sacral Fractures: Classification, Clinical Manifestations, Diagnosis, and Treatment
Aleksandr K.Orthopedic surgeon, MD
17 min read·September 02, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
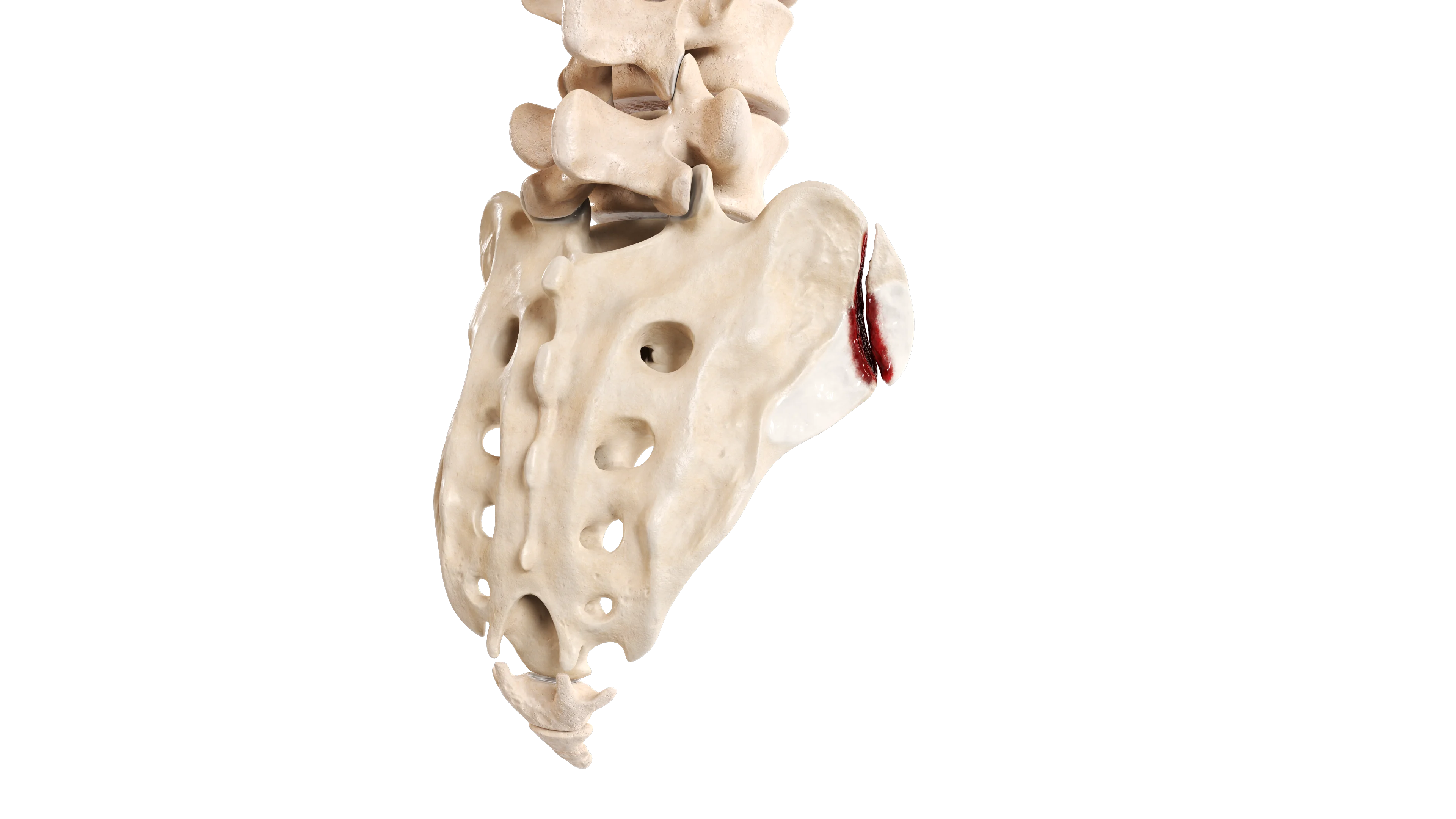
The sacrum is a triangular bone composed of five fused vertebrae, located between the two hip bones. Superiorly, it articulates with the fifth lumbar vertebra; inferiorly, it connects to the coccyx.
Sacral fractures range from simple, stable injuries to complex, unstable fractures with potential neurological risk (neurological complications occur in up to 25 % of cases).
Etiology
These fractures may have different etiologies, including non-traumatic mechanisms:
High-energy injuries: road traffic accidents, falls from significant heights.
Low-energy injuries: particularly in elderly patients with osteoporosis or metabolic bone disorders.
Pathologic fractures: due to tumor infiltration or prior radiation therapy.
Stress fractures: seen in athletes as a result of repetitive loading.
There are two primary mechanisms of sacral injury:
Direct trauma: a strong impact to the pelvis or lower back.
Indirect trauma: force transmitted through the femur to the pelvis during injury.
Sacral fractures are frequently associated with pelvic ring injuries and may be accompanied by fractures of the lumbar spine or acetabulum.
Epidemiology
They typically occur as part of a complex pelvic ring injury (in 30–45 % of cases). These fractures are most commonly observed in two distinct patient populations:
Younger individuals exposed to high-energy trauma (e.g., collisions).
Older adults, especially women, following low-energy trauma (often as a complication of osteoporosis).
Classification of Sacral Fractures
Several classification systems exist, but the most widely used is the Denis classification, which is based on the anatomical relationship to the sacral neural foramina.
Denis Classification
This system divides sacral fractures into three anatomical zones, each associated with distinct risks and clinical features.
Anatomical Zones of Sacral Fractures According to Denis Classification
Zone
Location
Zone 1
Lateral to the neural foramina. Accounts for approximately 50 % of sacral fractures. Neurological complications occur in about 5 % of cases, typically involving the L5 nerve root
Zone 2
Through the neural foramina. These fractures may be stable or unstable. Displaced fractures are generally unstable. Unstable fractures carry a high risk of nonunion, potentially resulting in poor functional outcomes
Zone 3
Medial to the foramina (central canal). Neurological complications are observed in up to 60 % of cases. These fractures are frequently associated with injuries to the bowel and bladder
Zone 3 fractures may be either longitudinal or transverse. These can be further subdivided into 4 types:
Type 1: Only kyphotic angulation at the fracture site (without displacement).
Type 2: Kyphotic angulation with anterior displacement of the distal sacrum.
Type 3: Kyphotic angulation with complete offset of the fracture fragments.
Type 4: Comminuted S1 segment (usually due to axial compression).
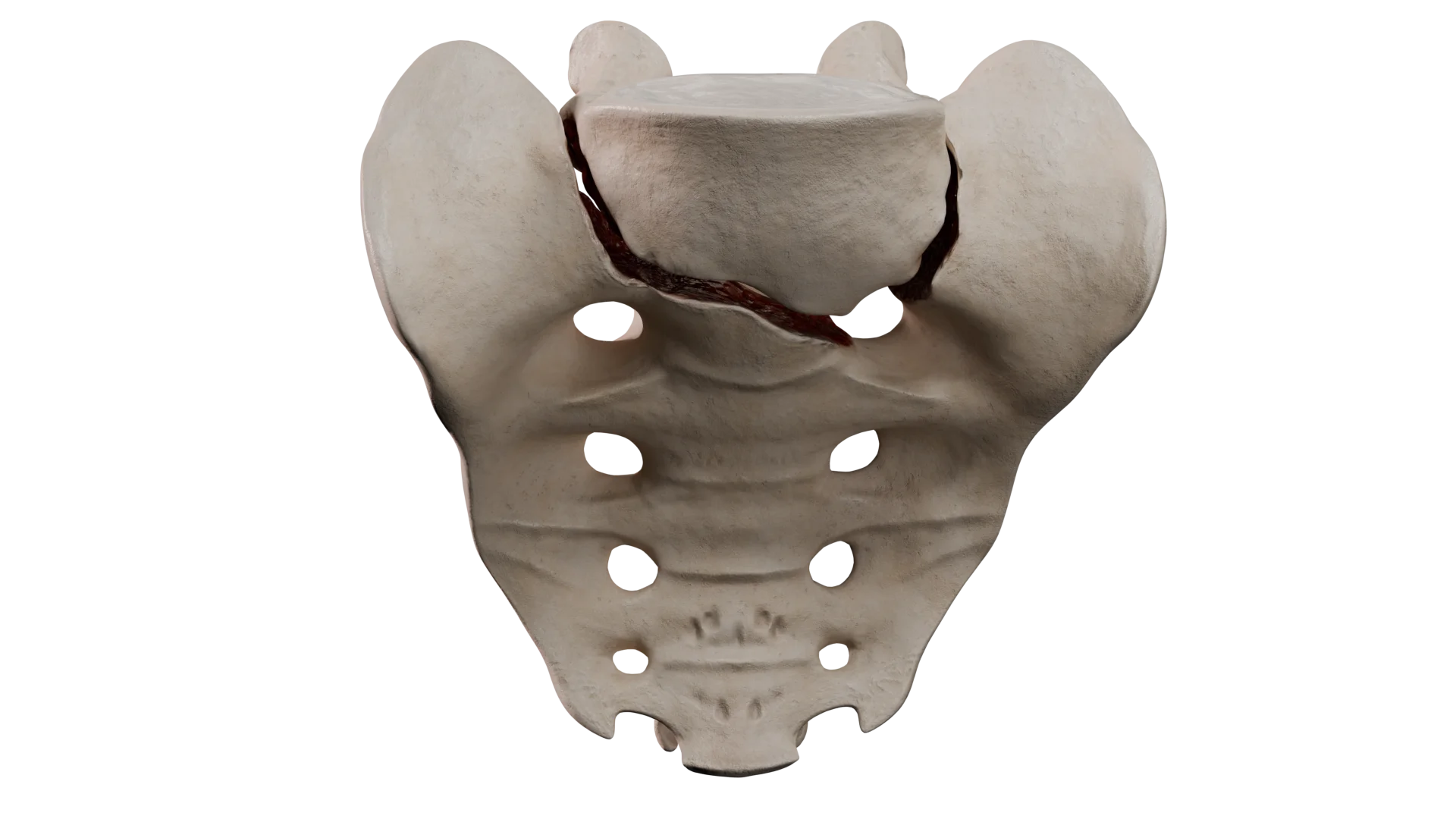
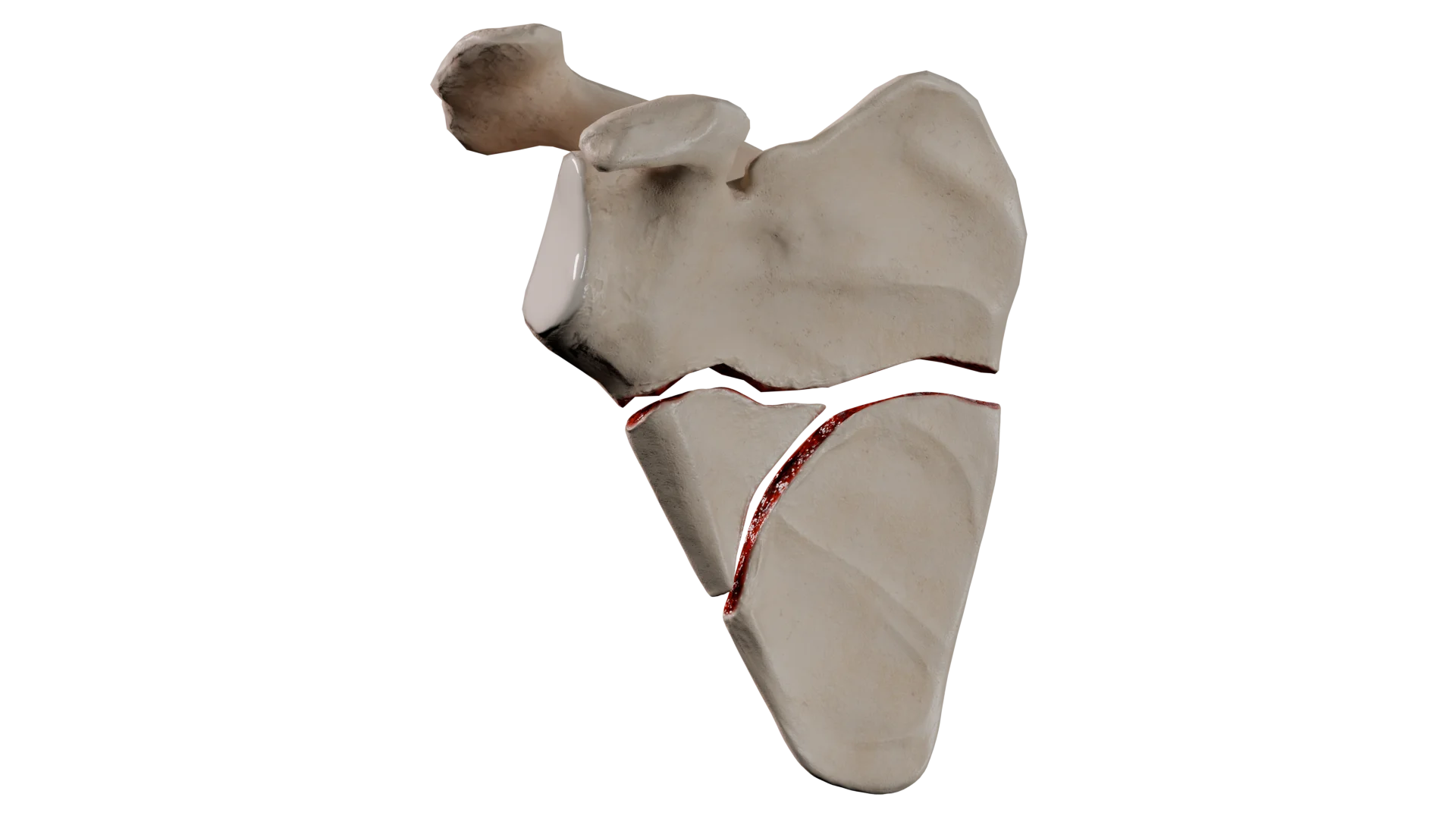
Transverse Sacral Fracture Without Displacement (Zone 3, Type 1 Fracture) — 3D-Model3D-Animation: Transverse Sacral Fracture
Zone 3 fractures may also be classified by morphology based on the fracture pattern:
H-shaped;
Lambda (ʎ)-shaped;
T-shaped;
U-shaped.
Thus, the U-shaped fracture, caused by axial loading of the sacrum, leads to spinopelvic dissociation and is often accompanied by neurological injury. According to the Denis classification, this corresponds to a Zone 3, Type 4 fracture.
The Isler classification describes sacral fractures that involve the lumbosacral junction. It defines three types of fractures:
Type 1 — fracture line lateral to the L5–S1 articular surfaces.
Type 2 — Fracture line traversing the L5–S1 articular surface.
Type 3 — Fracture line medial to the L5–S1 articular surface.
The Isler classification is particularly useful for detailed profiling of Zone 2 fractures under the Denis classification.
Diagnosis of Sacral Fractures
Diagnosis is based on clinical evaluation and radiologic imaging.
Clinical Evaluation
Medical History: Trauma or fall, pain localized to the lower back or pelvis.
Physical Examination: Local pain, swelling, sacral deformity, bruising, tenderness on pelvic manipulation, possible neurological deficits (e.g., weakness, numbness). In women, a pelvic examination may be performed to rule out open injuries; a rectal examination is also indicated.
Radiologic methods
Radiography: This modality may fail to detect sacral fractures, especially those without displacement (sensitivity up to 30 %).
Computed Tomography (CT): Considered the gold standard, CT accurately identifies fracture morphology, displacement, and involvement of neural structures.
Magnetic Resonance Imaging (MRI): The method is useful for evaluating nerve or soft tissue injury and for diagnosing stress fractures.
Clinical presentation
Typical clinical manifestations of sacral fractures include:
Pain: Localized to the lower back, buttocks, or pelvis; exacerbated by movement or weight lifting.
Swelling and Ecchymosis: Over the sacral region.
Neurological Signs: May include numbness, weakness, and bowel or bladder dysfunction (typically associated with Zone 2 and Zone 3 fractures due to sacral nerve involvement).
Associated Injuries: Pelvic ring disruption, fractures of the lower extremities, and visceral trauma.
Treatment of Sacral Fractures
Non-surgical treatment
A conservative approach in sacral fractures includes:
Pain control with analgesics.
Bed rest and limited weight-bearing, followed by gradual mobilization using crutches or support canes.
Physical therapy to restore adjacent joint mobility and muscle strength.
Indications for conservative management include:
Stable fractures (without displacement or with displacement up to 1 cm, isolated, without neurological deficits).
Stress fractures in osteoporotic patients without displacement.
Absence of associated pelvic ring instability.
Most low-energy, stable sacral fractures heal well with conservative treatment.
Surgical therapy
Surgical therapy in sacral fractures includes:
Open reduction and internal fixation (ORIF) using plates, screws, sacroiliac or lumbopelvic fixation.
Percutaneous sacroiliac screw fixation.
Decompression: Indicated in cases of neurological compromise.
Indications for surgical therapy include:
Unstable fractures or those associated with pelvic ring disruption.
Fractures with displacement greater than 1 cm.
Neurological deficits due to compression of nerve roots or the cauda equina (commonly in Zone 2 and Zone 3 fractures).
Open fractures or polytrauma requiring early mobilization.
Timely surgical intervention aims to stabilize the pelvis, relieve neurological compression, and enable early active rehabilitation.
Prognosis in Sacral Fracture
The prognosis following a sacral fracture is multifactorial and primarily depends on the anatomical type of fracture and the chosen treatment strategy.
Conservative management is generally suitable for Zone 1 fractures and select Zone 2 fractures. Long-term complications are uncommon, though some patients may develop chronic pain.
Surgical management provides fracture stability and reduces the risk of nonunion. However, it carries risks such as postoperative infection and hardware failure or migration. Infection at the surgical site and hardware migration significantly increase the likelihood of fracture nonunion. Zone 3 fractures typically require surgical intervention. In patients with neurological symptoms, early decompression may improve outcomes. Nevertheless, persistent neurological deficits are relatively common.
Thus, most patients with Zone 1 fractures return to their baseline activity level with favorable outcomes. Zone 2 fractures may cause long-term sensory and motor deficits in the lower limbs, though many patients regain full daily function through consistent rehabilitation. Up to 60 % of patients with Zone 3 fractures may experience persistent neurological impairments, often affecting their bowel, bladder, or sexual function.
Metabolic bone diseases, such as osteoporosis, are unfavorable prognostic indicators due to delayed or incomplete fracture healing. Concurrent damage to bone and soft tissue structures also impairs recovery and functional outcomes. Timely surgical intervention in cases of neurological deficits is critical for optimal therapeutic results.
Summary of Rehabilitation Potential and Prognosis Following Sacral Fractures by Zone
Fracture Type
Neurological Risk
Rehabilitation Potential
Prognosis
Zone 1
Low
Generally favorable
Most patients recover with conservative therapy
Zone 2
Moderate
Good, if nerves are preserved or decompressed
Prognosis varies; some patients may experience neurological deficits
Zone 3
High
Variable; increased risk of chronic pain and disability
Guarded prognosis; possible impairment of bladder, bowel, and sexual function
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Rehabilitation following Sacral Fracture
Rehabilitation following a sacral fracture is highly individualized. Its duration and focus depend largely on the type and severity of the fracture, presence of neurological deficits, surgical interventions, and patient-specific factors (e.g., age, comorbidities).
Primary goals include promoting fracture healing, restoring mobility, preventing complications, and addressing neurological deficits when present.
Summary of Rehabilitation Phases Following Sacral Fracture
Phase 3
Primary Objectives
Protocol
Acute (Weeks 0–2 post-injury or surgery)
To control pain and edema, prevent complications
Gentle movements in unaffected joints. Breathing exercises
Subacute (Weeks 2–6)
To initiate mobilization, maintain joint range of motion, preserve muscle tone
Isometric exercises. Standing under pain control. Gait training with walking aids
Recovery (Weeks 6–12)
To restore lost function, rebuild muscle endurance and strength, improve load tolerance
Progressive resistance training. Balance and proprioception exercises. Gait training
Functional (Months 3–6+)
To return to work, sports, and daily activities
Mobility-focused exercises. Functional and task-specific training for occupational and athletic demands
Rehabilitation Following Conservative Treatment (Stable Fractures)
When managed conservatively, stable sacral fractures require strict limitations on weight-bearing during the first 2 weeks post-injury. From Week 2, sitting in bed is permitted under pain control. By Weeks 3–4, standing with specialized aids is allowed.
Exercises focus on maintaining and restoring strength in the lower limbs and core. High-impact activities targeting the lower limbs should be avoided; closed-chain cardio (e.g., stationary cycling) is preferred. Stretching is also an essential component of the rehabilitation process.
Rehabilitation Following Surgical Treatment (Unstable Fractures)
Displaced or unstable sacral fractures require surgical intervention. Early postoperative rehabilitation aims to protect the surgically stabilized sacral segment. Weight-bearing is determined by the degree of stability achieved and the type of osteosynthesis.
To prevent contractures in the lower limb joints, in-bed, unloaded exercises are recommended. Gradual mobilization and standing using orthopedic aids should be encouraged under pain control.
Loading may be increased between Weeks 6–12 once fracture consolidation is confirmed radiographically. Subsequent training focuses on restoring gait and returning to daily activities, occupational tasks, and sports.
Neurorehabilitation is critical in cases of persistent neurological impairment. Key components include both physical and occupational therapy. It is also essential to strengthen unaffected muscle groups and prevent decubitus ulcers in areas of sensory loss. Orthopedic aids should be used during movement. Patients should be trained to manage their bowel and bladder, if needed. Functional electrical stimulation (FES) may be employed to enhance activation in partially denervated muscles.
Patient education is essential for improving adherence to the rehabilitation regimen. Early, consistent rehabilitation focused on restoring mobility, strength, and functional independence yields optimal outcomes — especially when coordinated by a multidisciplinary team.
FAQ
1. What are the main signs and symptoms of a sacral fracture?
The hallmark symptom is pain localized to the lower back, buttocks, and pelvis, which intensifies with movement. Additional signs may include localized swelling and hematoma (bruising). If nerve roots are involved, neurological symptoms may be observed, such as numbness, leg muscle weakness, and impaired bowel or bladder function.
2. What are the long-term consequences of a sacral fracture?
Outcomes depend directly on the fracture zone. Zone 1 fractures generally have a favorable prognosis. Zone 2 fractures may result in residual sensory or motor deficits in the lower limbs. Zone 3 fractures carry the highest risk, with up to 60 % of patients experiencing persistent neurological deficits, including impaired bowel, bladder, or sexual function.
3. How long does it take for a sacral fracture to heal?
Healing time is highly individualized. According to rehabilitation protocols, active recovery with progressive loading typically begins between Weeks 6–12, once radiographic signs of fracture consolidation appear. Moreover, full functional recovery — enabling return to sports or physically demanding work — may take 3 to 6 months or longer.
4. When and how can an individual start walking again after a sacral fracture?
Ambulation is strictly limited in the early phase. For stable fractures managed conservatively, lower limb loading is restricted during the first 2 weeks. Patients may begin standing with crutches or a walker between Weeks 3 and 4 post-injury. The entire mobilization process must be gradual and conducted under pain control.
5. Is side-lying permitted after a sacral fracture?
This article does not provide explicit guidance on permissible prone positions, such as side-lying. It emphasizes the importance of bed rest and minimizing body-weight loading only. Positional changes should be at physician’s discretion, based on the type and stability of the specific fracture.
References
1.
VOKA Catalog.
https://catalog.voka.io
2.
Oguzkaya S, Güvercin YS, Kızkapan TB, Eken G, Arat F, Misir A. Fracture lines and comminution zones of traumatic sacral fractures. Ulus Travma Acil Cerrahi Derg. 2023 Feb;29(2):247-251.
3.
Pascal-Moussellard H, Hirsch C, Bonaccorsi R. Osteosynthesis in sacral fracture and lumbosacral dislocation. Orthop Traumatol Surg Res. 2016 Feb;102(1 Suppl):S45-57.
4.
Beckmann NM, Chinapuvvula NR. Sacral fractures: classification and management. Emerg Radiol. 2017 Dec;24(6):605-617.
5.
Kweh BTS, Tee JW, Oner FC, Schnake KJ, Vialle EN, Kanziora F, Rajasekaran S, Dvorak M, Chapman JR, Benneker LM, Schroeder G, Vaccaro AR. Evolution of the AO Spine Sacral and Pelvic Classification System: a systematic review. J Neurosurg Spine. 2022 Jul 29;37(6):914-926.
6.
Gutierrez-Gomez S, Wahl L, Blecher R, Olewnik Ł, Iwanaga J, Maulucci CM, Dumont AS, Tubbs RS. Sacral fractures: An updated and comprehensive review. Injury. 2021 Mar;52(3):366-375.