Fractures of Cervical Spine: Classification, Symptoms, and Treatment
The article provides a detailed overview of C1 and C2 fractures. The etiology, classification, diagnostic methods, surgical management, and rehabilitation protocols are described.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
The clavicle is an S‑shaped bone that articulates with the sternum at the sternoclavicular joint and with the scapula at the acromioclavicular joint. Laterally, at its acromial end, it is flattened; the body is cylindrical, and the sternal end may be described as prismatic. It plays a key role in maintaining shoulder stability.
Clavicle fractures occur primarily as a result of direct or indirect trauma.
Most common causes include:
The primary mechanism of injury is a fall directly onto the lateral aspect of the shoulder, producing a compressive force that leads to fracture (seen in approximately 85 % of cases). Less commonly, the fracture may result from a direct blow to the clavicle or from indirect force transmitted through the arm.
Displacement of clavicular fragments is determined by the pull of muscles attached to the bone:
Clavicle fractures account for approximately 2.6–5 % of all fractures and up to 44 % of injuries to the pectoral girdle. They are most common in young, active individuals and children, with peak incidence in males aged 13–20 years.
The basic classification relies on the location of the fracture relative to the anatomical regions of the clavicle:
The high frequency of midshaft (middle 1/3) fractures is due to this region being the thinnest and narrowest portion of the clavicle and lacking ligamentous and muscular support.
The Neer classification is widely used in clinical practice to guide treatment decisions for fractures of the acromial (distal) end of the clavicle. It identifies five major fracture types and two subtypes.
| Neer Type | Fracture Characteristics | Recommended Treatment |
|---|---|---|
| Type I | Extra‑articular fracture. The fracture line runs laterally to the attachment of the coracoclavicular ligaments. Ligaments intact. Minimal displacement. Stable fracture | Medical |
| Type II | Extra‑articular fracture. The fracture line runs medially to the attachment of the coracohumeral ligaments. Ligaments intact. Significant medial displacement. Unstable fracture | Surgical. Nonunion rate with medical therapy may amount to 56 % |
| Type II | Extra‑articular fracture. Two anatomical patterns: 1. The fracture line runs through the ligament attachment (the conoid ligament disrupted, the trapezoid ligament intact). 2. The fracture line runs laterally to the ligament attachment, but the ligaments are injured. Significant medial displacement. Unstable fracture |
Surgical. Nonunion rate with medical therapy may amount to 30–45 % |
| Type III | Intra‑articular fracture. The fracture line runs laterally to the ligament attachment, extending into the acromioclavicular joint. Ligaments intact. Minimal displacement. Stable fracture | Medical. Risk of post‑traumatic acromioclavicular arthritis |
| Type IV | Extra‑articular fracture. In cases of open growth plates in the physeal region. Ligaments intact. Lateral clavicle fragment is displaced superiorly due to periosteal disruption. Stable fracture | Medical |
| Type V | Extra‑articular or intra‑articular fracture. Comminuted fracture. Ligaments intact. Significant medial displacement. Unstable fracture | Surgical |
3D-Models of Clavicle Fractures:
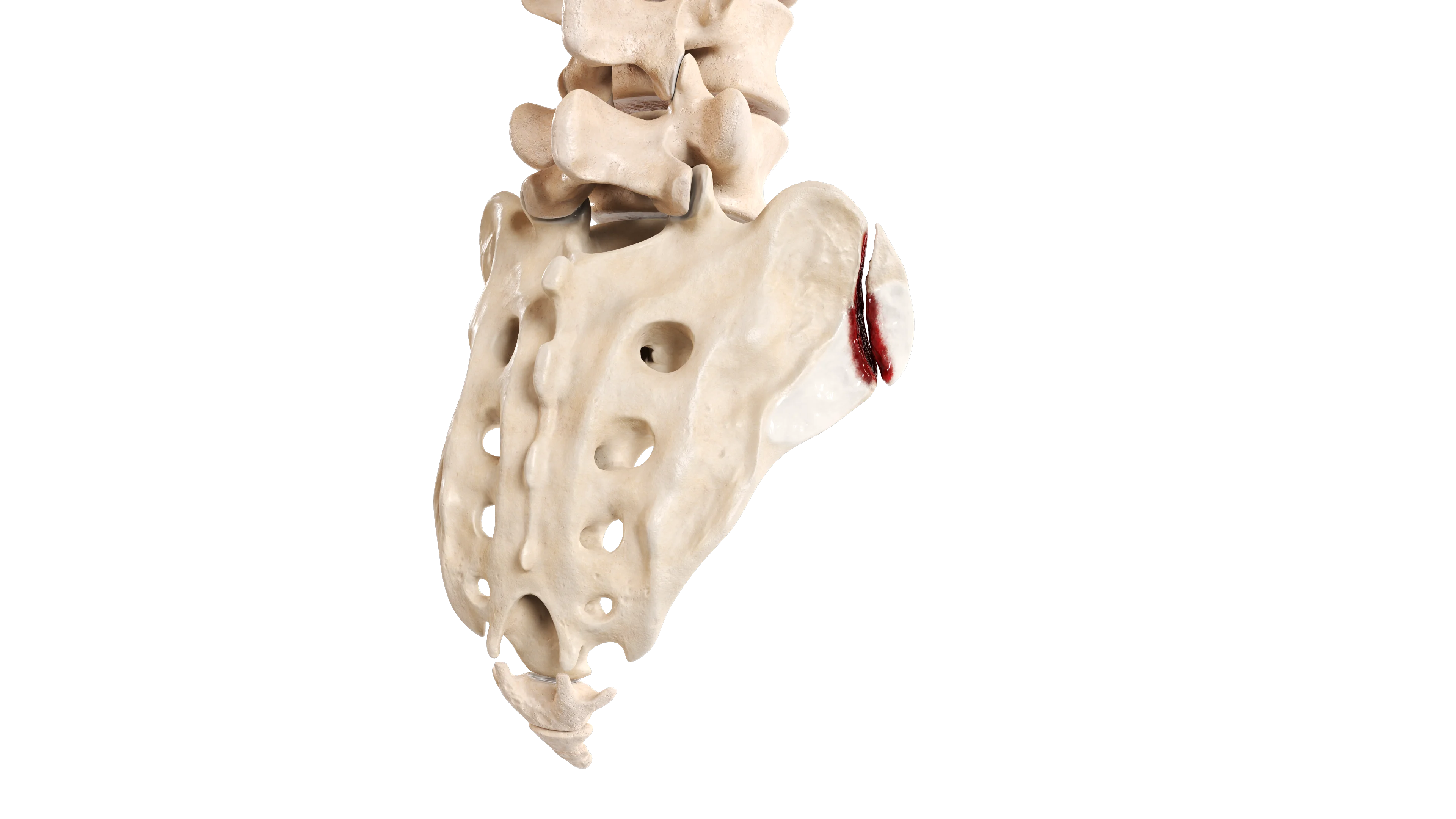
 Extra‑Articular Fracture of Sternal End of Clavicle
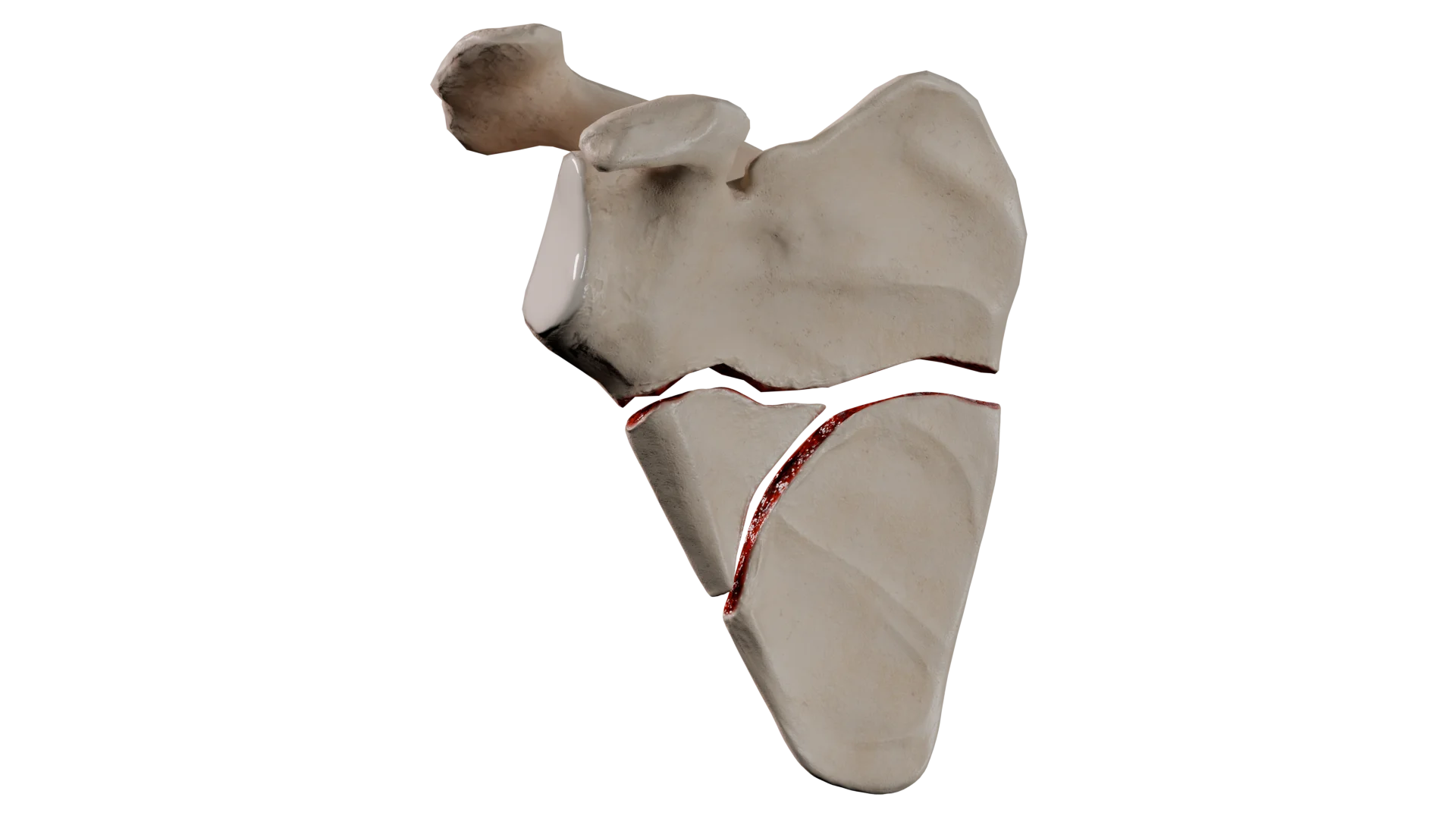
Extra‑Articular Fracture of Sternal End of Clavicle Comminuted Midshaft Fracture
Comminuted Midshaft Fracture Extra‑Articular Comminuted Fracture of Acromial End of Clavicle (Neer Type V)
Extra‑Articular Comminuted Fracture of Acromial End of Clavicle (Neer Type V)Typical clinical manifestations of clavicle fractures include:
Diagnosis is based on clinical evaluation and radiologic imaging.
Medical therapy is associated with a high rate of bone union in children and in minimally displaced fractures in adults.
Indications:
Procedure:
Surgery may provide earlier functional recovery and reduce the risk of nonunion or malunion in significantly displaced fractures.
Indications:
Procedure:
Rehabilitation follows a staged progression of orthopedic protection and gradually increasing load: immobilization (sling) → early passive motion → active motion → muscle strengthening → return to activity. The rate of progression depends on fracture type and treatment method.
| Timeline (Weeks) | Weight‑Bearing | Range of Motion | Notes |
|---|---|---|---|
| 0-2 | Contraindicated | Full range of motion is allowed for the elbow and wrist. Shoulder motion is contraindicated | Sling immobilization. Monitoring for vascular or visceral injury |
| 2-6 | Contraindicated | Pendular movements, passive shoulder flexion up to 90 ° (as tolerated) | – |
| 6-8 | Weight limit: up to 1 kg | Active shoulder motion > 90 ° (as tolerated) | Continued radiographic monitoring to assess fracture healing |
| 8-12 | Gradual increase in allowable load (as tolerated) | Full active shoulder range of motion. Isometric strengthening | – |
| 12+ | No restriction | No restriction | Continued radiographic monitoring to assess fracture healing. Sports activities may be resumed based on sport‑specific demands and radiographic evidence of union. |
| Timeline (Weeks) | Weight‑Bearing | Range of Motion |
|---|---|---|
| 0-2 | Contraindicated | Full range of motion is allowed for the elbow and wrist. Shoulder motion contraindicated |
| 2-6 | Contraindicated | Pendular passive movements (shoulder flexion not exceeding 90 °), progressing to active motion as tolerated |
| 6-8 | Gradual increase in load up to 3 kg | Full active shoulder range of motion. Isometric strengthening |
| 8-12 | Gradual increase in allowable load (as tolerated) | Full active shoulder range of motion. Exercises focus on restoring strength in the limb |
| 12+ | Complete | Return to daily activities Return to sports depends on the specific sport |
| Timeline (Weeks) | Weight‑Bearing | Range of Motion |
|---|---|---|
| 0-2 | Contraindicated. Sling immobilization | Full range of motion is allowed for the elbow and wrist. Pendular shoulder movements within a pain‑free range |
| 2-4 | Up to 1 kg | Abduction and flexion up to 90 ° assisted by the healthy arm as tolerated |
| 4-6 | Up to 2 kg | Progression to full active range of motion |
| 6-8 | Gradual increase in allowable load (as tolerated) | Progression to full active range of motion. Strengthening exercises |
| 8+ | No restriction | Gradual increase in exercise load. Return to sports no earlier than Week 12 |
| Timeline (Weeks) | Weight‑Bearing | Range of Motion |
|---|---|---|
| 0-2 | Contraindicated. Sling immobilization | Full range of motion is allowed for the elbow and wrist. Shoulder motion contraindicated |
| 2-6 | Up to 1 kg | Passive shoulder flexion and abduction up to 90 ° |
| 6-10 | Gradual increase in allowable load (as tolerated) | Active shoulder motion > 90 ° (as tolerated) Strengthening exercises |
| 10+ | No restriction | Return to sports once radiographic union is confirmed |
| Timeline (Weeks) | Weight‑Bearing | Range of Motion |
|---|---|---|
| 0-2 | Contraindicated. Immobilization in a soft sling | Full range of motion is allowed for the elbow and wrist. Shoulder motion contraindicated |
| 2-4 | Up to 1 kg | Passive pendular movements and passive flexion/abduction up to 90 ° |
| 4-6 | Up to 2 kg | Active shoulder motion > 90 ° (as tolerated) Strengthening exercises |
| 6-10 | Gradual increase in allowable load (as tolerated) | Full range of motion. Progressive strengthening without restrictions |
| 10+ | No restriction | Return to sports once radiographic union is confirmed |
General Requirements:
The process of returning to sport should be structured according to the timeline of the injury.
Load Progression by Phases:
Return to contact sports is permitted no earlier than 12 weeks after injury and only when fracture union is radiographically confirmed. Healing and recovery take more time in older adults, patients with metabolic disorders, and those who sustained high‑energy trauma. Children typically heal and recover more quickly.
Find more scientifically accurate content on our social media








The prognosis for clavicle fractures is generally favorable, although outcomes depend significantly on fracture location and treatment strategy.
1. How long does a clavicle fracture take to heal?
2. Why can the arm become numb after a clavicle fracture?
3. Is surgery always necessary for displaced fractures?
4. How should you sleep with a clavicle fracture?
5. What complications can occur after a clavicle fracture?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Moverley R, Little N, Gulihar A, Singh B. Current concepts in the management of clavicle fractures. J Clin Orthop Trauma. 2020 Feb;11(Suppl 1):S25-S30.
3.
Kang LX, Faulkner HJ, Howard WH, Low AK. Displaced medial clavicle fractures: a systematic review of outcomes after nonoperative and operative management. JSES Int. 2022 Oct 15;7(1):79-85.
4.
von Rüden C, Rehme-Röhrl J, Augat P, Friederichs J, Hackl S, Stuby F, Trapp O. Evidence on treatment of clavicle fractures. Injury. 2023 Oct;54 Suppl 5:110818.
5.
Yan MZ, Yuen WS, Yeung SC, Wing-Yin CW, Wong SC, Si-Qi WW, Tian E, Rashed S, Yung CSY, Fang CX. Operative management of midshaft clavicle fractures demonstrates better long-term outcomes: A systematic review and meta-analysis of randomised controlled trials. PLoS One. 2022 Apr 29;17(4):e0267861.
6.
Panagopoulos A, Solou K, Tatani I, Triantafyllopoulos IK, Lakoumentas J, Kouzelis A, Athanasiou V, Kokkalis ZT. What is the optimal surgical treatment for Neer type IIB (IIC) distal clavicle fractures? A systematic review and meta-analysis. J Orthop Surg Res. 2022 Apr 7;17(1):215.
7.
Wang C, Li X, Dong S, Xie W, Ling Z, Meng C, Stöckle U. Midshaft clavicle fractures with associated ipsilateral acromioclavicular joint injuries: a systematic review. BMC Surg. 2025 Feb 28;25(1):87.
8.
Yue L, Huang C, Zhang J, Wang Z, Wang S, Sun H. Treatment Strategies for Distal Clavicle Fractures: A Narrative Review. Orthop Res Rev. 2025 May 19;17:221-227.
9.
Kilkenny CJ, Daly GR, Whelehan SP, Vukanic D, Alrawashdeh M, Boland F, Quinlan JF, Molony DC. Return to play following clavicular fracture – A systematic review and meta analysis. JSES Rev Rep Tech. 2024 Dec 14;5(2):259-269.
Loading test 6 questions
Table of Contents




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io