Fractures of Cervical Spine: Classification, Symptoms, and Treatment
Aleksandr K.Orthopedic surgeon, MD
29 min read·January 29, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Fractures of the cervical spine are serious injuries that require thorough diagnosis and treatment. Injuries to the upper cervical spine — specifically the first (C1, atlas) and second (C2, axis) vertebrae — require even more caution as they provide head mobility and lie in close proximity to the brainstem and spinal cord.
Fracture of First Cervical Vertebra
The first cervical vertebra (C1, atlas) supports the skull and contributes to head movement. A fracture typically compromises the ring‑shaped structure of the vertebra. C1 fractures are clinically significant due to their proximity to the spinal cord and brainstem, creating a risk of neurological deficits or life‑threatening instability.
Etiology
C1 fractures are primarily associated with trauma.
High‑energy injuries: road traffic accidents, falls from height, or sports injuries (i.e., diving into shallow water).
Low‑energy injuries: in older adults (for example, a fall from standing height) due to metabolic bone disorders such as osteoporosis.
Rare causes: pathologic fractures due to tumors or infections.
Mechanism of Injury
The classic mechanism is axial loading, in which force compresses the skull and transmits energy to the atlas (C1), causing structural failure. Hyperextension or hyperflexion may aggravate the condition.
Epidemiology
C1 fractures account for 2–13 % of cervical spine injuries and 1–3 % of all spinal injuries. Men aged 20–40 years are more prone to such fractures (75 % of cases) due to high‑risk activities. A secondary peak occurs in older adults (> 65 years) with osteoporosis.
Mortality rates are low (4–10 %), but associated injuries (for example, C2 fractures) are observed in 30–50 % of cases.
Classification of C1 Fractures
Gehweiler and Dickman Classification
The Gehweiler classification describes five types of C1 fractures based on involvement of specific anatomical structures. The Dickman classification of injuries to the transverse atlantal ligament is also integrated into this system.
Gehweiler Classification with Dickman Modifications
Type
Description
Incidence
Type 1
Fracture of the anterior arch of the atlas
24%
Type 2
Fracture of the posterior arch of the atlas
22%
Type 3
Fracture of both anterior and posterior arches (Jefferson burst fracture)
34%
Subtype 3a
Intact transverse atlantal ligament
–
Subtype 3b (Dickman Type 1)
Disrupted transverse atlantal ligament
–
Subtype 3b (Dickman Type 2)
Bony avulsion at the ligament attachment with an intact transverse atlantal ligament
–
Type 4
Fracture of the lateral mass
19%
Type 5
Isolated fracture of the transverse process
1%
Landells Classification
Similar to the Gehweiler system, the Landells classification identifies three types of fractures:
Type I: Fracture confined to either the anterior or posterior arch.
Type II: Fracture of both arches.
Type III: Fracture of the lateral mass (extending into one arch only).
Stable fractures: localized neck pain, stiffness, and muscle spasm.
Unstable fractures: possible neurological deficits (limb weakness, impaired respiration) due to compression of the spinal cord or brainstem.
Vertebral artery injury (blunt cerebrovascular injury, BCVI): may present with dizziness (vertigo), double vision (diplopia), vision loss, uncoordinated movements (ataxia), difficulty swallowing (dysphagia), or vomiting.
Asymptomatic cases: may occur in some patients and complicate diagnosis.
Diagnosis of C1 Fracture
Diagnosis is based on clinical evaluation and radiologic imaging.
Clinical Evaluation
In general, neck pain and restricted motion are the primary symptoms of cervical spine injuries. During the neurological examination, motor and sensory deficits are assessed. With isolated C1 injuries, neurological deficits are less likely; however, C2 fractures are associated with a significantly higher risk of neurological complications.
Radiologic Methods:
CT (computed tomography): the gold standard for detecting fracture lines and displacement.
Radiography: an open‑mouth anteroposterior view may demonstrate lateral displacement of the lateral masses (displacement greater than 7 mm suggests a Jefferson fracture).
MRI (magnetic resonance imaging): allows evaluation of ligamentous injury and spinal cord compression.
During evaluation of a C1 injury, possible developmental anomalies of the atlas should be considered. A split or bipartite atlas is a rare congenital anomaly in which the atlas is divided into two halves by fusion defects in both the anterior and posterior arches. The bony defects are covered by fibrous tissue. The defects in both cases are located along the midline; however, the anomaly of the anterior arch is typically smaller than the defect of the posterior arch. A bipartite atlas is asymptomatic and usually identified incidentally on imaging.
Treatment of C1 Fractures
Medical Therapy
Indications: stable fractures (intact transverse ligament, no displacement).
Procedure:
Immobilization: rigid cervical collar (e.g., Miami J) or a halo-gravity traction device (HGTD) for 8–12 weeks.
Dynamic radiographic monitoring: serial imaging assists with alignment and fracture healing.
Rehabilitation: physical therapy after immobilization to restore mobility and muscle tone.
3D Animation — Stable Types of C1 Fractures According to Gehweiler (Gehweiler J., Duff D., Martinez S., Miller M., Clark W., 1976)
Surgical therapy
Indications: segmental instability (transverse ligament rupture, displacement > 7 mm), neurological deficits, or failure of medical therapy. The goal is to prevent spinal cord injury and restore spinal alignment.
Procedure:
Occipitocervical fusion: stabilizes the skull and cervical spine. Typically performed in combined C1 and C2 injuries.
C1–C2 fusion: preserves some neck motion while fixing the atlas to the axis.
3D Animation — Unstable Types of C1 Fractures According to Gehweiler (Gehweiler J., Duff D., Martinez S., Miller M., Clark W., 1976)
Fracture of Second Cervical Vertebra
The second cervical vertebra (C2, axis) plays a key role in supporting the skull, enabling head rotation, and protecting the upper spinal cord. Fractures in this region range from minor nondisplaced cracks to severe, unstable injuries that endanger the spinal cord and vital functions.
Etiology
C2 fractures may result from various traumatic mechanisms:
Direct trauma: the most common cause, often due to high‑impact injuries.
Road traffic accidents: both high‑speed impacts and lower‑energy mechanisms such as abrupt deceleration.
Sports injuries: contact sports, diving accidents, and equestrian activities.
Pathologic conditions: metastatic lesions of C2 and chronic metabolic disorders affecting bone density, contributing to low‑energy fractures.
Mechanism of Injury
Because of its unique anatomical structure, С2 is susceptible to characteristic injury patterns and fracture types:
Hyperextension: a sudden backward movement of the head (for example, a rear‑impact collision) may cause a “hangman’s fracture” — a bilateral fracture of the pars interarticularis.
Axial loading: vertical force applied to the head (for example, diving into shallow water) may result in fractures of the odontoid process (dens axis).
Flexion‑rotation: twisting forces may also produce fractures of the odontoid process or the lateral mass.
Direct trauma: blows to the upper neck or viscerocranium may lead to C2 fractures.
Epidemiology
C2 fractures account for 20 % of all cervical spine fractures.
Odontoid (dens) fractures are the most common (50–75 %), particularly in older adults after falls from standing height.
Hangman’s fractures (traumatic spondylolisthesis of the axis) are the second most common C2 fracture type and are frequently associated with road traffic accidents and falls.
They tend to be more common in men involved in athletic activities or occupations with higher injury risk (construction, etc.).
Classification of С2 Fractures
Multiple classification systems exist for C2 fractures. Historically, the most significant systems are based on the anatomical region involved. For example, Schatzker classified fractures according to their position relative to accessory ligaments.
Classification of Odontoid Fractures (Anderson & D’Alonzo)
The most widely used classification for odontoid fractures is based on the position and location of the fracture.
Anderson and D’Alonzo Classification with Handley Modification*
Type
Description
Description
Type 1
Oblique fracture of odontoid process tip (essentially an avulsion fracture of the alar ligament)
Rare; considered a stable fracture (however, atlanto‑occipital instability must be excluded using functional flexion‑extension radiographs)
Type 2 Type 2a
Fracture at odontoid process base and neck
The most common and potentially unstable fracture. High rates of nonunion are associated with disrupted local blood supply
Type 3
Fracture extending into the vertebral body, often involving the articular surface of the atlantoaxial joint
More favorable healing potential compared with Type 2
*The Hadley subclassification identifies the comminuted variant of Type 2 fractures. This subtype carries a significantly increased risk of nonunion with medical therapy. Occurs in 5–10 % of all Type 2 fractures.
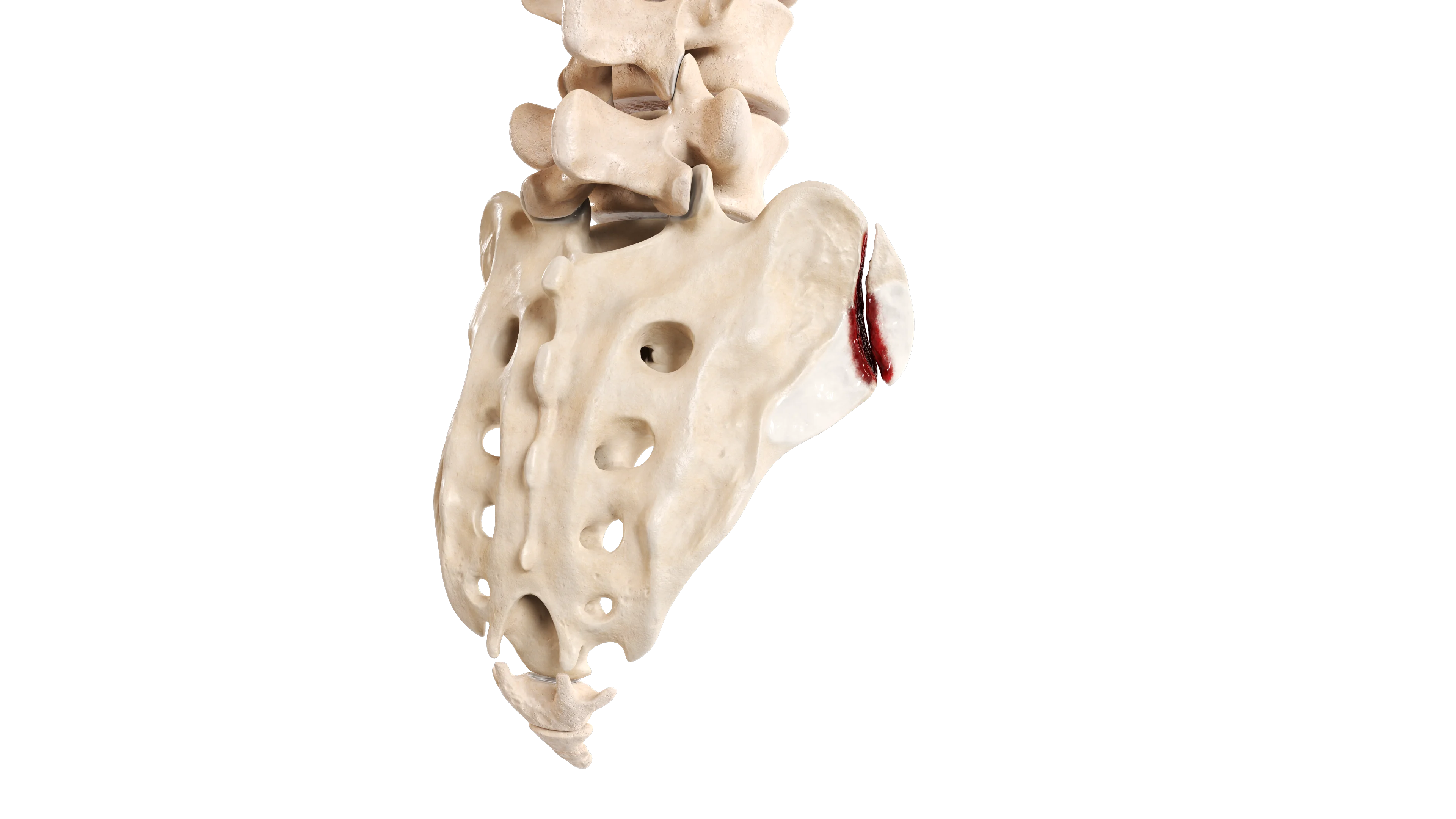
Odontoid fracture, Type 2a (Anderson and D’Alonzo, Hadley modification)
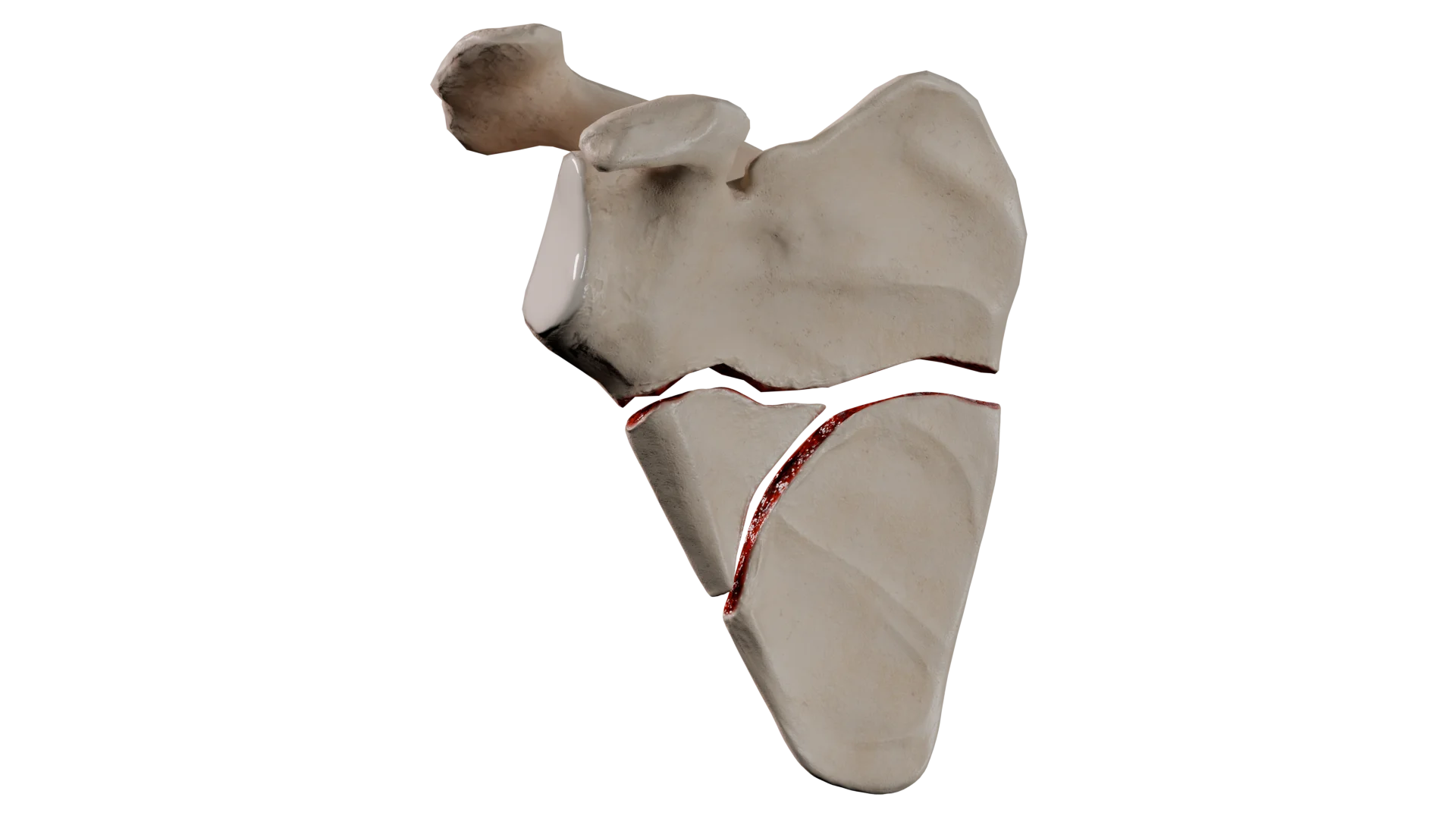
Odontoid fracture, Type 3 (Anderson and D’Alonzo)
3D Animation — Odontoid Fracture Types According to Anderson & D’Alonzo (Anderson L. & D’Alonzo R., 1974)
Grauer classification is a more detailed system for Type 2 odontoid fractures (subtypes A, B, C), based on the shape and direction of the fracture line, guiding treatment strategy.
The Roy — Camille classification does not adequately describe the direction of fragment displacement or the course of the fracture line.
An embryologic classification has also been developed based on the embryologic fusion centers of the odontoid process. While Type 1 involves the upper quarter of the dens, Type 2 affects its lower three quarters.
Classification of Hangman’s Fractures (Levine & Edwards)
This system was developed for fractures of the pars interarticularis of C2 (traumatic spondylolisthesis of the axis, hangman’s fracture) based on the mechanism of injury.
Levine and Edwards Classification
Type
Mechanism
Description
Treatment
Type 1
Axial compression and hyperextension
Horizontal displacement of fragments < 3 mm, no angular displacement, C2–C3 intervertebral disc intact. Stable fracture
Medical (rigid cervical collar for 4–6 weeks)
Type 2
Hyperextension and axial loading followed by flexion
Horizontal displacement > 3 mm, angular displacement up to 10 °, vertical fracture line, C2–C3 intervertebral disc disrupted, posterior longitudinal ligament disrupted. Unstable fracture
Displacement < 5 mm: reduction with traction, then HGTD immobilization (6–12 weeks). Displacement > 5 mm: surgical treatment
Type 2а
Flexion and distraction
No horizontal displacement, significant angular displacement (> 11 °), horizontal fracture line
Traction is contraindicated. Reduction is achieved with gentle axial loading and hyperextension, followed by HGTD immobilization (6–12 weeks)
Type 3
Flexion and distraction followed by hyperextension
Type 1 fracture with associated bilateral C2–C3 facet joint dislocation
Surgical
Clinical presentation
Severe neck pain: localized to the upper cervical spine, worsened by movement.
Reduced range of motion in the neck.
Occipital headache: may occur due to referred pain.
Neurological symptoms: rare, but may include numbness, weakness, or even quadriplegia in severe injuries.
Difficulty breathing and swallowing: may occur in cases of a large retropharyngeal hematoma.
Diagnosis
Diagnosis is based on clinical evaluation and radiologic imaging.
Clinical Evaluation:
Medical history: recent neck trauma, mechanism of injury, neurological symptoms.
Physical examination: neck pain, tenderness on palpation, restricted motion, and possible neurological deficits including limb weakness, numbness, or respiratory impairment.
Radiologic Methods:
Radiography: standard anteroposterior, lateral, and open‑mouth odontoid views (the latter being more reliable) help identify odontoid fractures. Functional radiographs (flexion and extension): required to assess atlanto‑occipital instability.
CT (computed tomography): the gold standard; provides detailed visualization of fracture morphology and displacement.
MRI (magnetic resonance imaging): indicated when neurological deficits are present.
Treatment of C2 Fractures
Medical Therapy
Indications: nondisplaced fractures, no spinal cord compression and no progressive neurological symptoms. Also indicated for patients who cannot undergo surgery.
Procedure:
Rigid cervical collar: commonly used for nondisplaced Type 1 and Type 3 odontoid fractures, as well as Type 1 traumatic spondylolisthesis.
HGTD immobilization: provides maximal external stabilization; typically required for some Type 2 odontoid fractures and certain traumatic spondylolistheses.
Many C2 fractures can be managed conservatively, especially when stable and without neurological deficits. Most patients recover with appropriate immobilization: external brace or HGTDs achieve 100 % union in Type 1 fractures and 85–100 % union in Type 3 fractures. In Type 2 fractures, union rates reach 57 %, but this rate decreases significantly in older adults.
Surgical therapy
Indications: instability, displacement, nonunion, neurological deficit, or multiple injuries.
Procedure:
Anterior odontoid screw fixation: internal fixation for displaced Type 2 odontoid fractures, especially in younger patients. Union is achieved in approximately 90 % of cases.
Posterior C1–C2 fusion: indicated for unstable, comminuted fractures or failed medical therapy. Fusion rates are high, although the preferred surgical technique plays a significant role.
Surgical intervention often provides excellent stabilization and neurological outcomes but carries operative risks and requires longer rehabilitation.
Prognosis and Outcomes
Key prognostic factors for C1 and C2 fractures include integrity of the ligamentous structures, degree of displacement and angulation, timing and effectiveness of stabilization, and bone quality. Structured and consistent rehabilitation also plays an important role in overall recovery.
Prognosis in C1 Fracture
Isolated fracture of the anterior arch: favorable due to stability and rare neurological complications.
Isolated fracture of the posterior arch: similar prognosis; the fracture is stable, and neurological complications are extremely rare.
Combined fracture of the anterior and posterior arches: prognosis depends on the integrity of the transverse ligament. With an intact transverse ligament (Gehweiler Type 3A), the fracture is relatively stable and the prognosis is relatively favorable. With any form of transverse ligament injury, there is a risk of chronic instability and reduced cervical range of motion after fracture healing.
Fracture of the lateral mass: prognosis also depends on ligamentous involvement. With an intact transverse ligament and stable immobilization, the prognosis is favorable. With ligamentous injury, there is a risk of segmental instability, sometimes requiring spinal fusion.
Isolated fracture of the transverse process: favorable prognosis, but evaluation of nearby vascular structures is required.
Prognosis in C2 Fracture
Fractures of the odontoid process tip: favorable prognosis due to high union rates, fracture stability, and rare neurological complications.
Fracture of the odontoid process base: associated with a high risk of nonunion due to anatomical features of the blood supply, reaching 50 % with medical therapy. Malunion and chronic pain syndrome are possible. Thus, the prognosis for odontoid base fractures is less favorable.
Type 3 fractures (Anderson and D’Alonzo): good prognosis because the fracture line passes through well‑vascularized cancellous bone of the vertebral body and is more stable than Type 2 fractures. Union is achieved in 85–90 % of cases.
Prognosis for traumatic spondylolisthesis(hangman’s fracture) depends on fracture morphology, i.e., stability. Stable fractures have a favorable prognosis. Unstable fractures require surgical treatment, increasing the risk of complications. Neurological complications are rare because the spinal canal widens in this injury pattern. Union is achieved in approximately 90 % of cases. Chronic pain syndrome typically develops with misdiagnosis, delayed treatment, or nonunion.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Rehabilitation Protocol
Rehabilitation is a key stage of treatment. It is divided into phases depending on fracture stability.
If new neurological symptoms appear during rehabilitation, existing symptoms worsen, body temperature rises above normal, or breathing/swallowing becomes difficult, immediate medical evaluation is required.
Rehabilitation After C1 Fracture
For Stable Fractures (Medical Therapy):
Phase 1 — Immobilization (0–6 weeks): Stable fixation (brace/HGTD). Cervical loading and movement are strictly limited. Isometric exercises in healthy segments and extremities, as well as breathing exercises, are permitted.
Phase 2 — Early Mobilization (6–12 weeks): Initiated after radiographic confirmation of fracture consolidation. Exercises aimed at restoring range of motion and strength. Load and movement volume should increase gradually, as tolerated. It is advisable to begin with flexion‑extension movements, followed by rotational and lateral bending exercises.
Phase 3 — Functional Recovery (12+ weeks): Return to unrestricted daily activities. Contact sports and high‑impact axial loading should be avoided. Cardiovascular training, swimming, range‑of‑motion exercises, and progressive strengthening of cervical and upper thoracic muscles are acceptable.
If neurological symptoms appear or recur, or if fracture consolidation is delayed, the duration of each phase is determined at physician’s discretion.
Rehabilitation After Unstable Fractures (Postoperative Period):
0–6 weeks: Protection with a device (brace/HGTD). Breathing exercises, bed mobility training, and gait training under immobilization are indicated.
6–12+ months: Return to work, progressive physical loading, and practice of task‑specific skills.
6–12 weeks: Protected mobilization; strengthening of the back and limb muscles to enable independent ambulation and daily activities.
12–24 weeks: Restoration of range of motion (within the limits permitted by the hardware). Exercises focus on strengthening the core and anterior abdominal wall. Cycling is permitted.
Rehabilitation After C2 Fracture
Rehabilitation Protocol for Stable Fractures
Phase
Precautions
Protocol
Immobilization (0–6/8 weeks)
Immobilization in a cervical brace or HGTD
Breathing exercises, active limb movements. Bed mobilization. Upright positioning as tolerated
Mobilization (6–12 weeks)
Gradual discontinuation of a cervical brace
Cervical spine movements as tolerated. Strengthening of upper thoracic and cervical muscles. Balance and proprioception training
Functional Recovery (12+ weeks)
High‑intensity loading must be avoided until complete fracture consolidation
Increasing range of motion in the injured segment Return to daily activities, restoration of work capacity, and training of required specific skills
Rehabilitation Protocol for Unstable C2 Fractures Requiring Surgical Treatment
Phase
Precautions
Protocol
Early Postoperative Period (0–6 weeks)
Immobilization of the operated segment, preventing motion
Breathing exercises. Active limb movements. Bed mobilization. Upright positioning as tolerated
Early Mobilization (6–12 weeks)
Discontinuation of immobilization after radiographic confirmation of positive healing dynamics
Strengthening of paraspinal and limb muscles Increasing range of motion as permitted by the hardware Exercises aimed at restoring balance and posture
Functional Recovery (12+ weeks)
Limiting range of motion and loading depending on the type of fusion
Progressive strengthening of cervical and upper thoracic muscles Aerobic training. Return to daily activities Restoration of work capacity
The degree of motion restriction depends on the type of surgical intervention. Fixation of the odontoid process with a screw preserves rotation at the operated segment. By contrast, posterior C1–C2 fusion results in loss of rotation at that level. Occipitocervical fusion leads to significant limitations in segmental mobility.
FAQ
1. What is a Jefferson fracture?
It is a “burst” fracture of the first cervical vertebra (the atlas, C1), involving fractures of both the anterior and posterior arches. It occurs due to a strong axial load (for example, a blow to the head).
2. How dangerous are cervical spine fractures, and can they be fatal?
Injuries to the upper cervical spine (C1–C2) are dangerous because of their proximity to the brainstem and respiratory centers. Severe injuries may be fatal. However, many isolated fractures occur without neurological deficits and are successfully treated.
3. What is a HGTD?
It is a metal frame attached to the skull with pins and connected to a chest vest. It provides the most rigid cervical immobilization, allowing complex fractures to be treated without surgery.
4. Can a cervical fracture go unnoticed?
Yes, especially in older adults with osteoporosis. Sometimes a fracture (for example, an odontoid fracture) causes only moderate pain, which may be mistaken for a bruise or an exacerbation of a degenerative disease. Therefore, after any head or neck trauma in older adults, diagnostic imaging (CT or X‑ray) is necessary.
5. What are the possible consequences of a C2 fracture?
Outcomes depend on the fracture type. Possible consequences include complete recovery, limited head rotation (after fusion), chronic pain, or neurological deficits (including paralysis).
6. Is surgery mandatory for an odontoid fracture?
Surgery is most often required for Type 2 fractures (fracture at the base of the odontoid process), as they heal poorly with medical therapy. Fractures of the tip (Type 1) and the body (Type 3) are usually treated conservatively.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Meyer C, Eysel P, Stein G. Traumatic Atlantoaxial and Fracture-Related Dislocation. Biomed Res Int. 2019 Mar 18;2019:5297950.
3.
Chan KS, Shlobin NA, Dahdaleh NS. Diagnosis and management of isolated C1 fractures: A systematic review. J Craniovertebr Junction Spine. 2022 Jul-Sep;13(3):233-244.
4.
Shin JW, Suk KS, Kim HS, Yang JH, Kwon JW, Lee HM, Moon SH, Lee BH, Park SJ, Park SR, Kim SK. Direct Internal Fixation for Unstable Atlas Fractures. Yonsei Med J. 2022 Mar;63(3):265-271.
5.
Tu Q, Chen H, Li Z, Chen Y, Xu A, Zhu C, Huang X, Ma X, Wang J, Zhang K, Yin Q, Xu J, Xia H. Anterior reduction and C1-ring osteosynthesis with Jefferson-fracture reduction plate (JeRP) via transoral approach for unstable atlas fractures. BMC Musculoskelet Disord. 2021 Aug 30;22(1):745.
6.
Shin JJ, Kim KR, Shin J, Kang J, Lee HJ, Kim TW, Hong JT, Kim SW, Ha Y. Surgical Versus Conservative Management for Treating Unstable Atlas Fractures: A Multicenter Study. Neurospine. 2022 Dec;19(4):1013-1025.
7.
Mathkour M, Cardona JJ, Chaiyamoon A, Glynn RM, Jenkins S, Graham RA, Johal J, Gardner B, Iwanaga J, Dumont AS, Tubbs RS. Classifications of Odontoid Process Fractures: A Systematic Review and Proposal of a New Simplified Classification System Based on Embryology. Cureus. 2022 Dec 14;14(12):e32520.
8.
Gornet ME, Kelly MP. Fractures of the axis: a review of pediatric, adult, and geriatric injuries. Curr Rev Musculoskelet Med. 2016 Dec;9(4):505-512.
9.
Mohile NV, Kuczmarski AS, Minaie A, Syros A, Geller JS, Maaieh MA. Management of combined atlas and axis fractures: a systematic review. N Am Spine Soc J. 2023 Apr 24;14:100224.
10.
Al-Mahfoudh R, Beagrie C, Woolley E, Zakaria R, Radon M, Clark S, Pillay R, Wilby M. Management of Typical and Atypical Hangman’s Fractures. Global Spine J. 2016 May;6(3):248-56.