Choroid Plexus Tumors: Papilloma and Carcinoma — Etiology, Classification, and Treatment
Artemiy G.Neuro-oncological surgeon, MD
11 min read·December 11, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
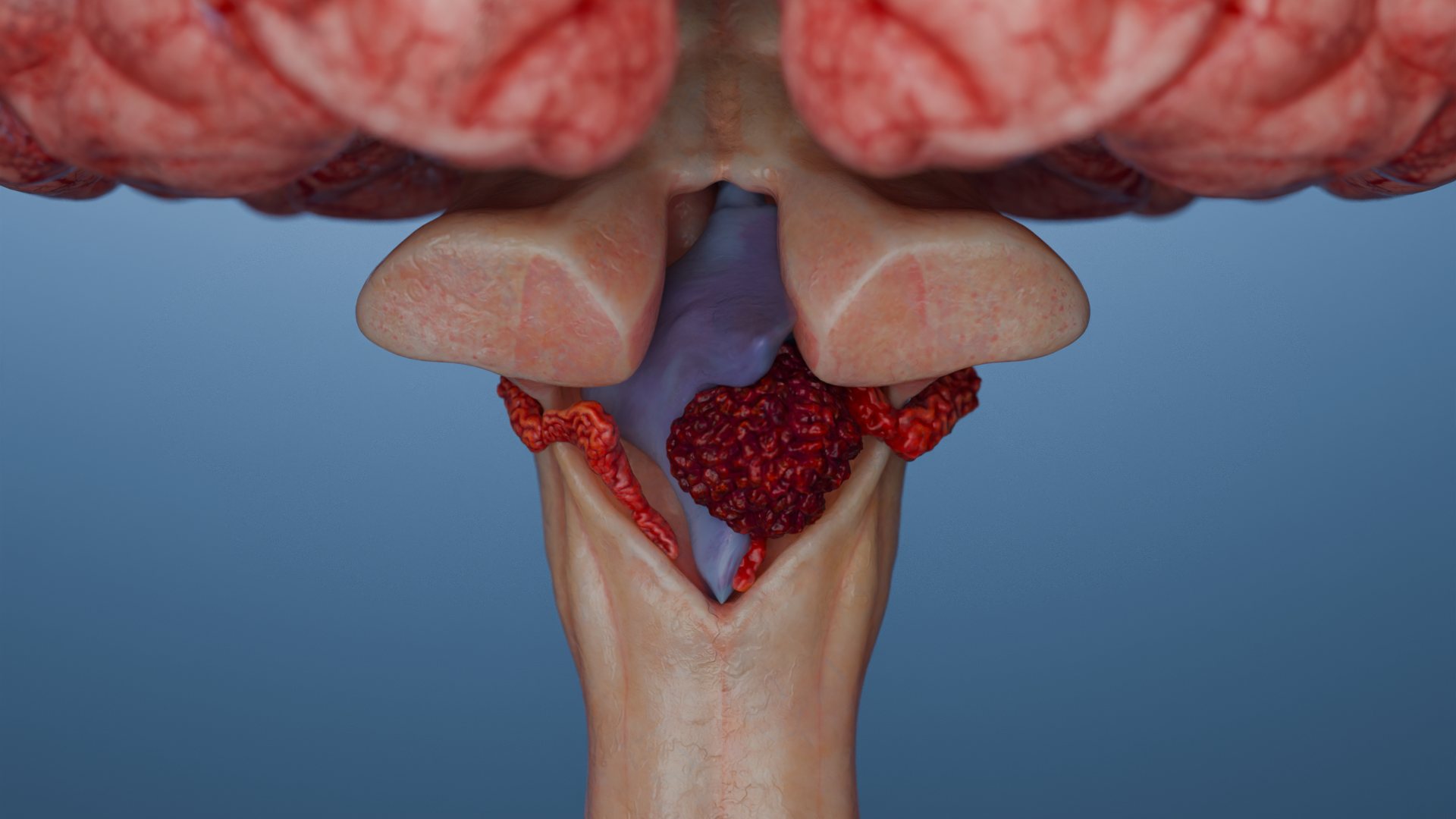
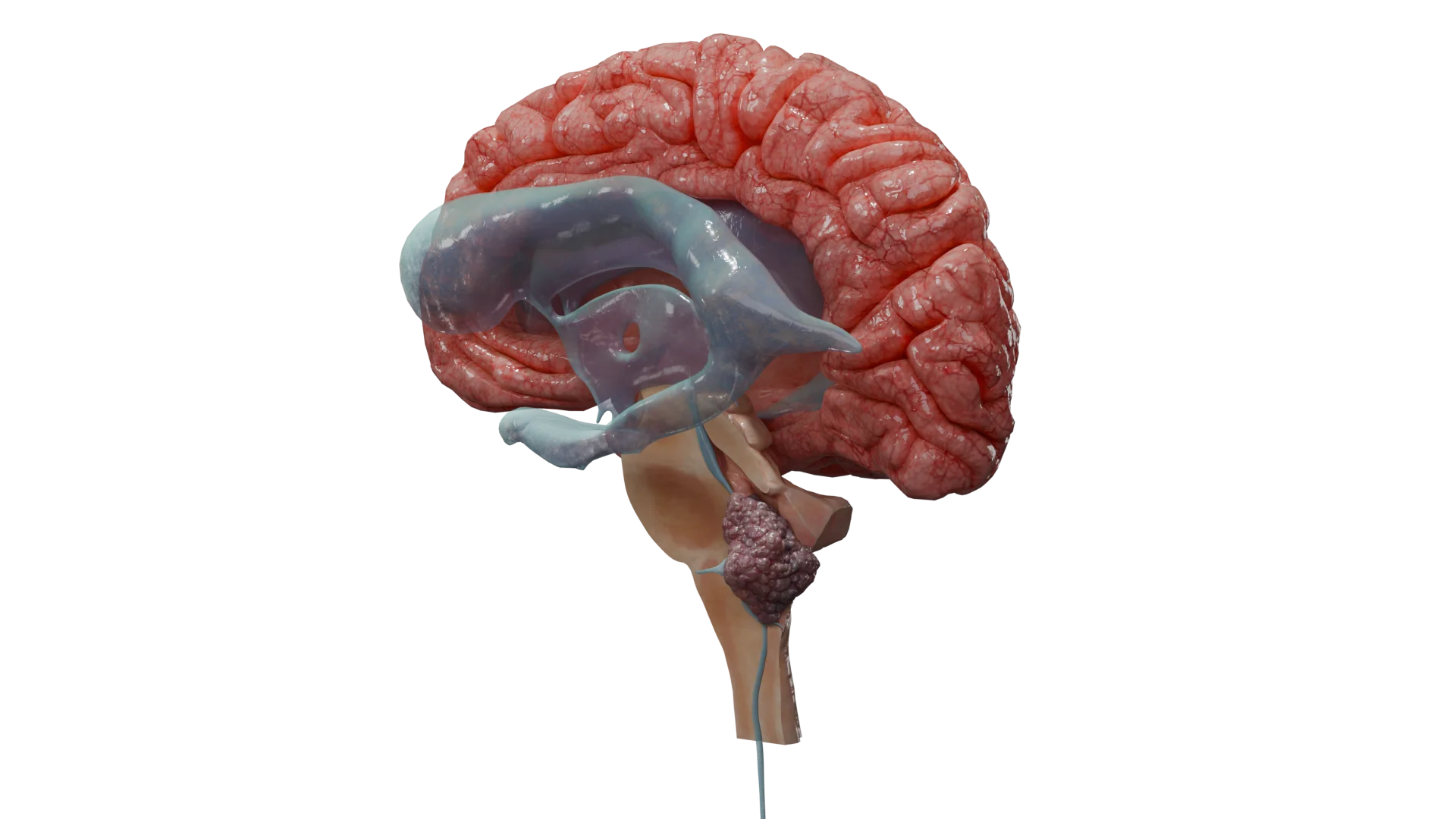
The choroid plexus produces cerebrospinal fluid (CSF) and is located within the ventricles of the brain. Tumor localization is age-related: the lateral ventricles are more commonly affected in children, while in adults, the tumors are generally found in the fourth ventricle.
Choroid plexus papilloma (CPP) is a benign epithelial tumor of the choroid plexus. According to the WHO classification, it is designated Grade 1. Note that it is the most common type of choroid plexus tumors.
Choroid plexus carcinoma (CPC) is a rare, highly malignant tumor (WHO Grade 3) arising from the epithelium of the choroid plexus within the brain ventricles. It is most frequently diagnosed in children under 5 years of age. CPC is characterized by aggressive growth, invasion, CNS metastasis, and an extremely poor prognosis.
Etiology and Epidemiology of Choroid Plexus Tumors
Etiology and Genetic Factors
The exact causes of CPP remain unknown. CPP is not typically associated with specific driver mutations, but some cases are linked to rare genetic syndromes, such as Aicardi syndrome.
Atypical CPP (aCPP) and malignant CPC: These forms may arise in association with TP53 mutations, especially in children with Li — Fraumeni syndrome (LFS).
Up to 60 % of CPC patients harbor somatic TP53 mutations, while 40 % of cases are associated with germline TP53 mutations in LFS.
Other genetic alterations may involve PTEN and CDKN2A, which regulate cell cycle progression.
Epidemiology
Low incidence and strong age-related features are the main predictors of epidemiology of choroid plexus tumors.
Incidence: Choroid plexus tumors are rare, accounting for < 1 % of all intracranial tumors. In infants under 1 year, they represent 10–15 % of all intracranial neoplasms.
Age: Peak incidence occurs within the first three years of life.
Localization: In children, tumors are more often found in the lateral ventricles; in adults, in the fourth ventricle. Gender ratio: Approximately equal between males and females.
Clinical Manifestations and Symptoms of CPT
Primary symptom: Intracranial hypertension due to hydrocephalus (excess CSF production). It typically presents as headache; infants show progressive head enlargement.
Other symptoms: Nausea, vomiting, seizures, hemiparesis, lethargy, visual disturbances (depending on tumor location).
Rarely, intracranial hemorrhage may occur.
3D-Animation: Choroid Plexus Papilloma
Classification of Choroid Plexus Tumors
The current WHO Classification (5th Edition, 2021) is based on morphological, immunohistochemical, and molecular features of the tumors.
Recent studies identify three molecular subtypes based on methylation and gene expression:
Pediatric supratentorial low-risk (CPP/aCPP)
Pediatric supratentorial high-risk (CPC)
Adult infratentorial low-risk (CPP/aCPP)
Thus, clinical practice now integrates morphology, proliferative activity, molecular markers, and TP53 statusto determine prognosis and treatment strategy.
Diagnosis and Differential Diagnosis
Diagnostic Methods
MRI: Primary diagnostic tool. CT/Ultrasound: Used when MRI is unavailable (e.g., ultrasound in infants via the fontanelle).
MRI and CT: Hyperintense on T2 in MRI, calcifications on CT, intense contrast enhancement.
CPC: Heterogeneous structure, necrotic areas, invasion, intense contrast enhancement, signs of vasogenic edema around the tumor.
Molecular diagnostics: TP53 germline (LFS) screening is mandatory in CPC.
Lumbar puncture: Performed to exclude tumor cells in CSF (especially in CPC).
Thus, in children, differential diagnosis focuses primarily on ependymomas and embryonal tumors, while in adults, it is aimed at meningiomas and metastatic carcinomas.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment Methods and Prognostic Strategies for CPT
Management of these tumors is multimodal and begins with surgical intervention, which determines subsequent therapeutic strategy and overall prognosis.
1. Surgical therapy
Gold standard:Gross total resection (GTR).. Endoscopic techniques are commonly used.
CPP prognosis: Even subtotal resection of a typical CPP may yield favorable outcomes.
CPC challenges: Complete removal is often difficult due to invasion and intraoperative bleeding.
Postoperative care: CSF shunting may be required.
2. Radiation Therapy
CPP: Generally not required after radical resection.
Indications: Recurrent or atypical CPP, incomplete resection.
CPC: Patients > 3 years may receive craniospinal irradiation following chemotherapy.
Limitations: Avoided in children due to high cognitive impairment risk. In younger <(< 3 years) and LFS patients, this method is used with caution due to secondary tumor risk.
Regimens: Carboplatin/Etoposide/Vincristine (CarbEV); CycEV. CarbEV shows superior survival rates in CPC.
In some LFS cases, high-dose consolidation chemotherapy along with autologous bone marrow transplantation may be used.
Prognosis and Survival Factors
Favorable: Following complete resection of CPP/aCPP, 10-year survival exceeds 90 %. Recurrence rates in aCPP are higher; adjuvant (postoperative) therapy is more common.
Unfavorable: CPC has poorer outcomes, with 5-year survival around 40 %, especially in patients with TP53 mutations. Prognosis worsens with genetic syndromes, metastases, incomplete resection, and LFS.
FAQ
1. How does CPP differ from CPC?
Choroid plexus papilloma (CPP) is a benign tumor (WHO Grade 1) with favorable prognosis. Choroid plexus carcinoma (CPC), on the other hand, is a highly malignant (WHO Grade 3), aggressive neoplasm with poor prognosis.
2. What is the main symptom of CPTs?
CPT is marked by intracranial hypertension due to hydrocephalus. In infants, the condition is associated with head enlargement.
3. What is the role of TP53 mutation in CPC?
TP53 mutation has strong prognostic significance: it is often linked to Li — Fraumeni syndrome (LFS) and indicates poor outcome.
4. What is the gold standard treatment for CPP?
CPP is preferably managed through gross total surgical resection.
5. Why is radiation therapy avoided in young children with CPC?
Radiotherapy is generally not indicated in patients under 3 years due to high risk of severe cognitive impairment and secondary tumors, especially in LFS patients.
References
1.
VOKA Catalogue. [Electronic resource].
https://catalog.voka.io/
2.
Wolff JE, et al. “Final results of the Choroid Plexus Tumor study CPT-SIOP-2000.” J Neurooncol 2022;156(3):599–613.
3.
Louis DN, et al. “The 2021 WHO Classification of Tumors of the Central Nervous System: a summary.” Neuro Oncol. 2021;23:1231–1251.
4.
Thomas C, et al. “Molecular genetics and diversity of choroid plexus tumors.” Neuro-Oncol Adv 2024.
5.
Andour H, et al. “Atypical choroid plexus papilloma: Diagnosis and management.” SAGE Open Med. 2024; doi:10.1177/2050313X241254000.
6.
Yankelevich M, et al. “Marrow-ablative consolidation chemotherapy and molecular targeted therapy for CPC.” Neuro-Oncol Adv 2024;6(1):vdae109.
7.
Cornelius A, et al. “Molecular Guided Therapy Provides Sustained Clinical Remission in Pediatric CPC.” Frontiers Pharmacol. 2017;8:652.
8.
Wolff JE, Sajedi M, Brant R. “Choroid plexus tumours.” Br J Cancer. 2002 87:1086–91.
9.
Safaee M, et al. “Choroid plexus papillomas: advances in molecular biology and surgical management.” Neurosurg Focus. 2012;32(2):E6.
10.
Akade E, et al. “Diagnosis of choroid plexus papilloma.” Curr Probl Cancer. 2024; doi:10.1016/j.cpt.2023.09.005.