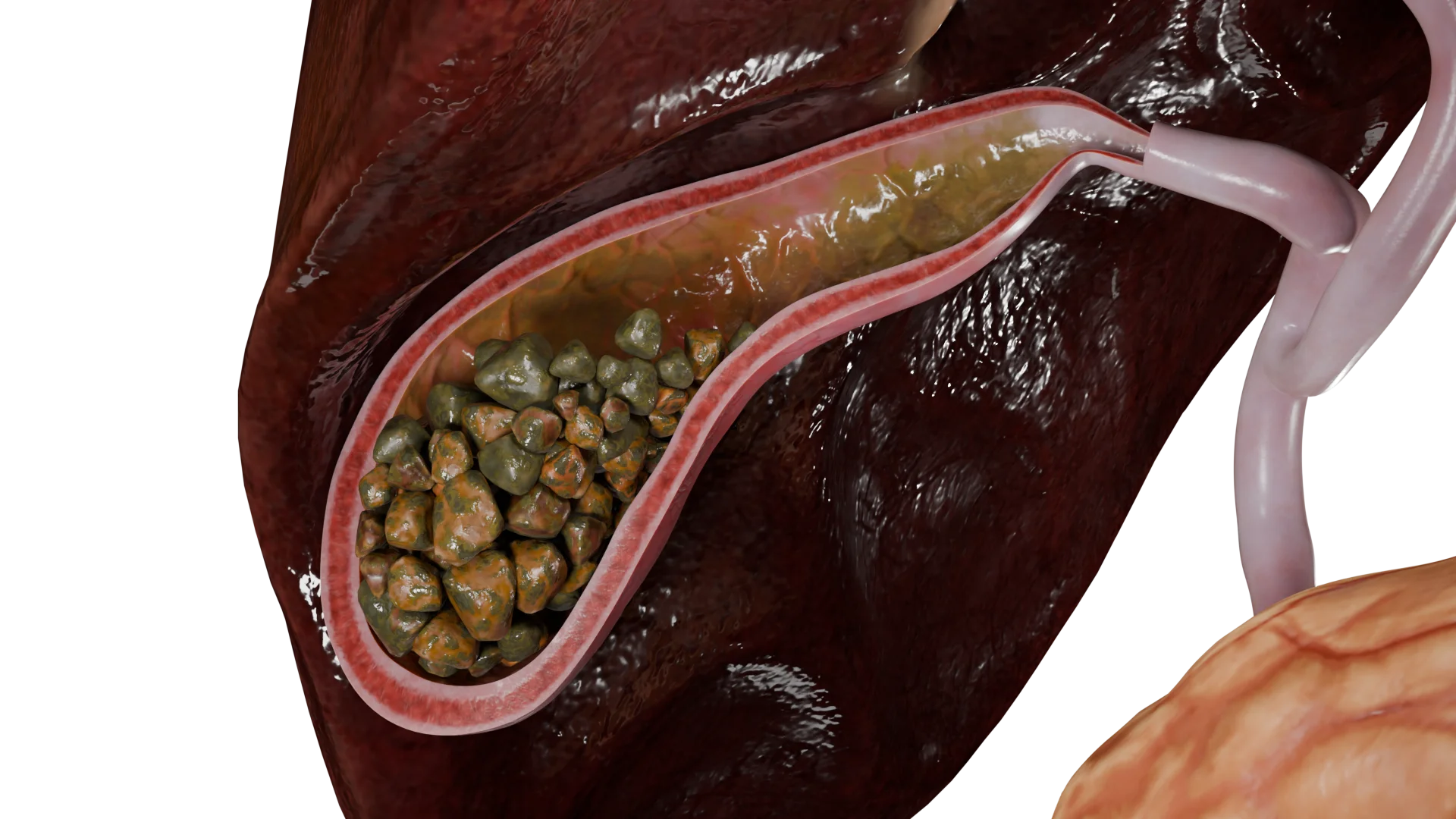
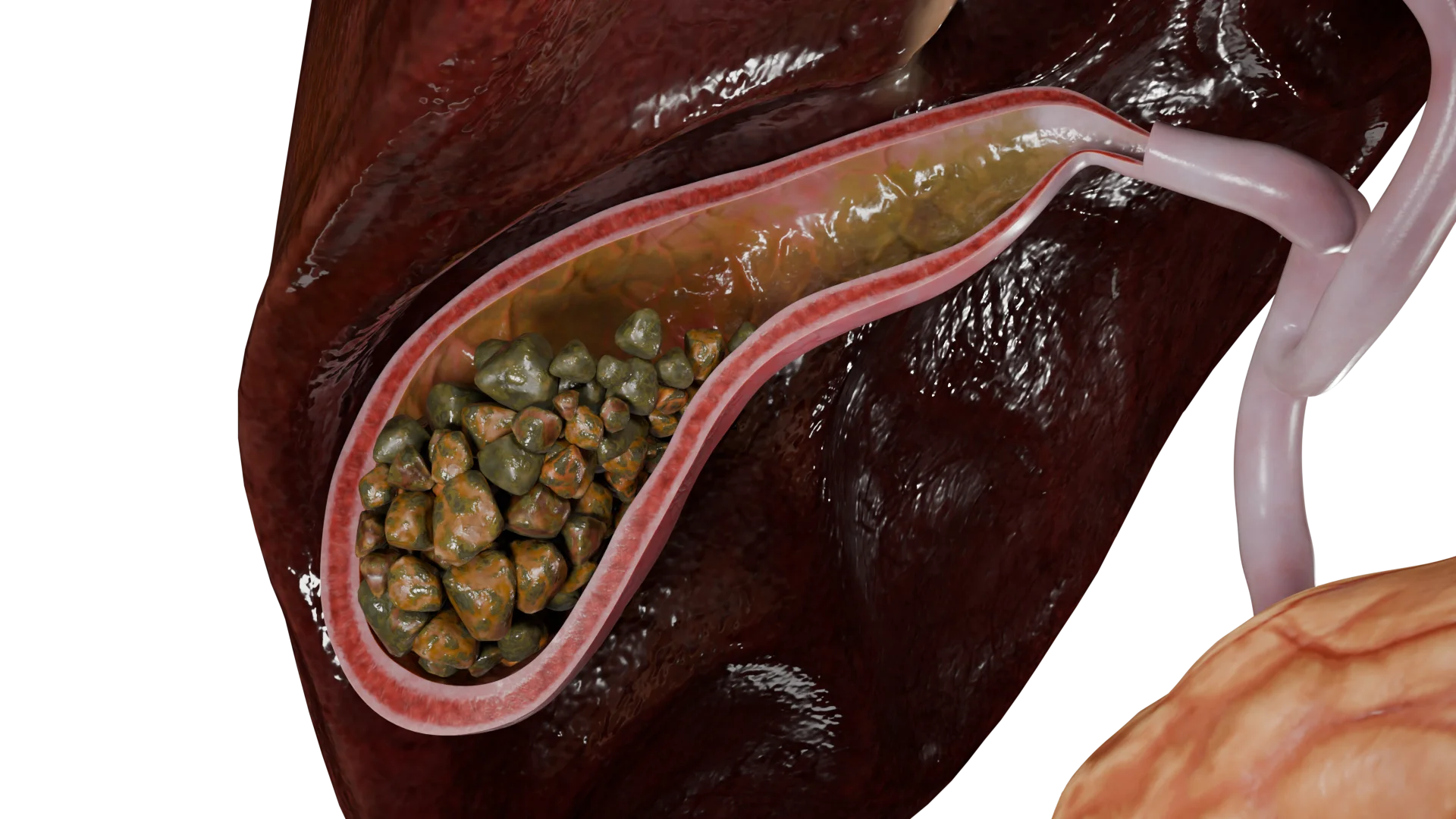
Gallstone disease (Cholelithiasis) is a multifactorial condition. It is characterized by bilirubin and cholesterol metabolism disorders with gallstones formation in the hepatobiliary system.Acute calculous cholecystitis (multiple mixed stones in the gallbladder with inflammation of its wall) – 3D Model
Gallstones risk factors
Cholelithiasis is associated with a range of risk factors. They include as follows:
Imbalanced diet. A diet high in trans fats, low-density lipoproteins (LDL), and very low-density lipoproteins (VLDL);
Low or a lack of physical activity;
Endocrine disorders accompanied by dyslipidemia;
Use of antiepileptic drugs;
Age;
Female sex;
Genetic predisposition;
Smoking and alcohol abuse;
Impaired bile outflow from the gallbladder.
Pathogenesis
Сalculi (stones) in the hepatobiliary system primarily associated with the presence of risk factors, which lead to the development of bile sludge.
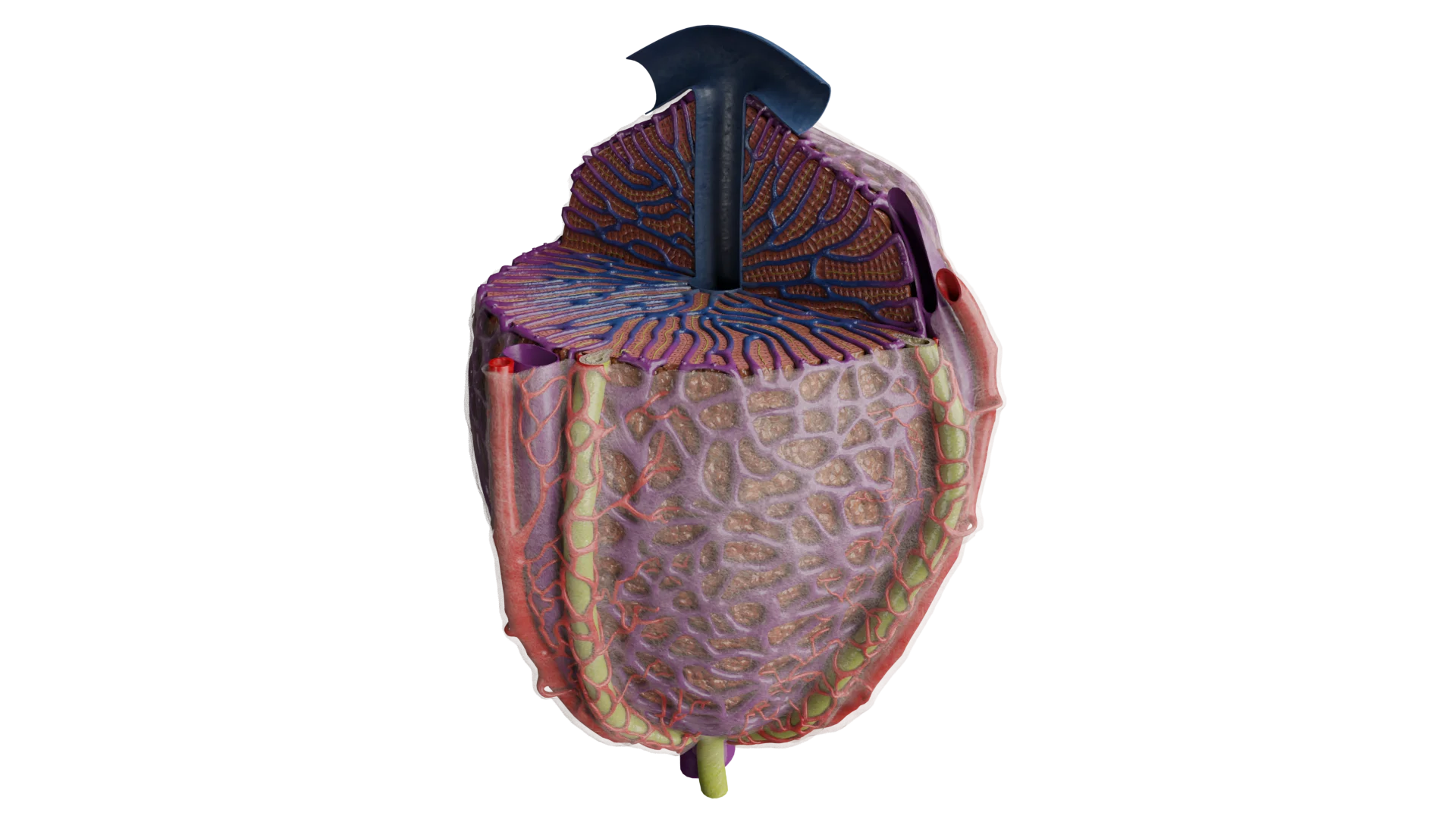
Bile consists of fractions of bile acids, such as cholic, chenodeoxycholic and deoxycholic acids, as well as phospholipids, proteins, bilirubin, bioactive compounds, metals (zinc, copper, magnesium, etc.), and ions of sodium, chlorine and potassium. The process of bile formation occurs in hepatocytes.
Structure of the hepatic lobule (acinus) – 3D Model
Through the excretory ducts of the hepatobiliary system, bile enters the duodenum, where it emulsifies dietary fats and activates the enzymatic systems of the gastrointestinal tract. In this process, the gallbladder serves as a bile reservoir.
Calculi are formed secondary to biliary sludge when bile becomes too dense due to an unbalanced bile composition or impaired bile outflow from the hepatobiliary system in high-risk patients. Biliary sludge syndrome is associated with an imbalance among the components of bile.
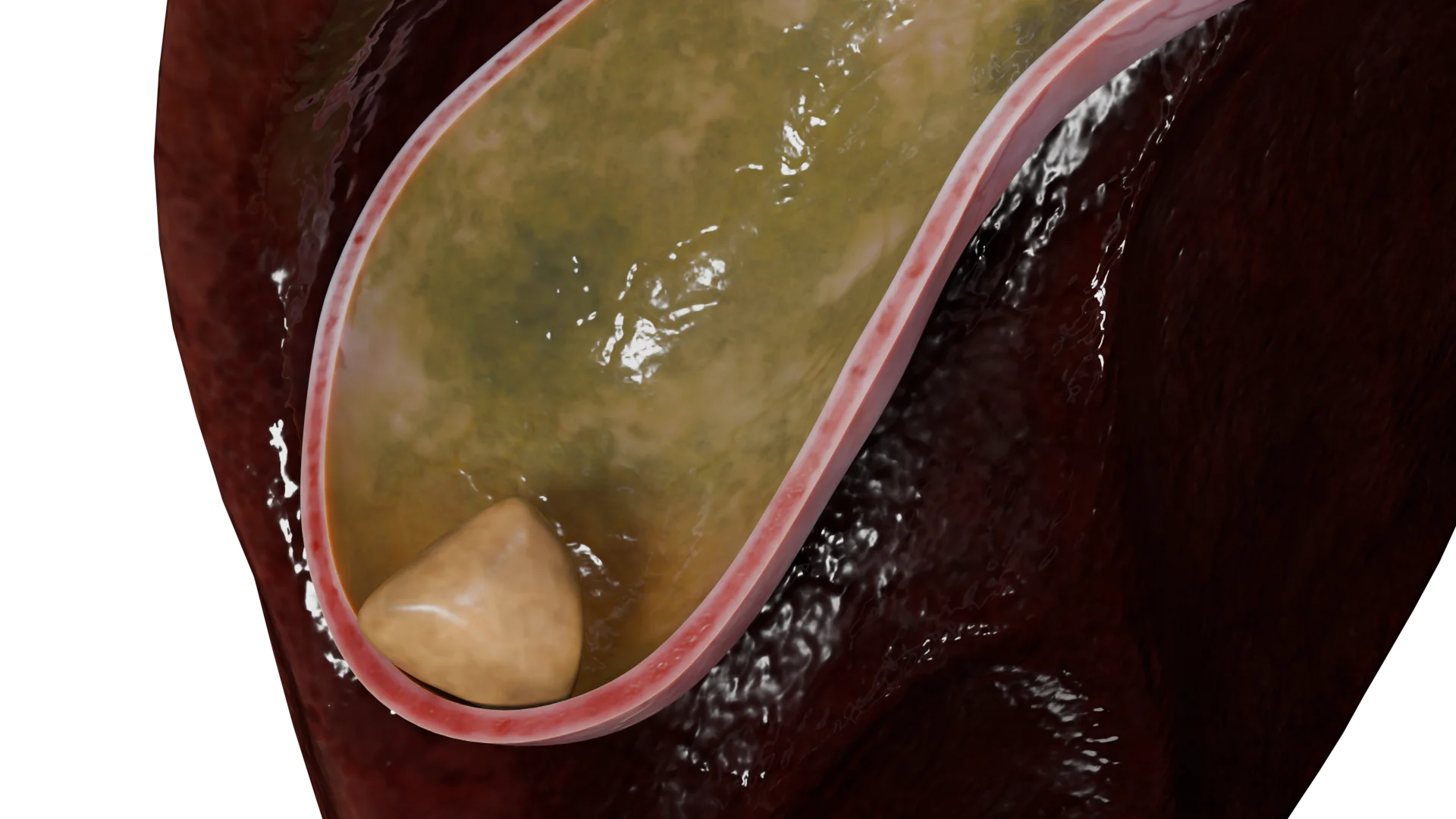
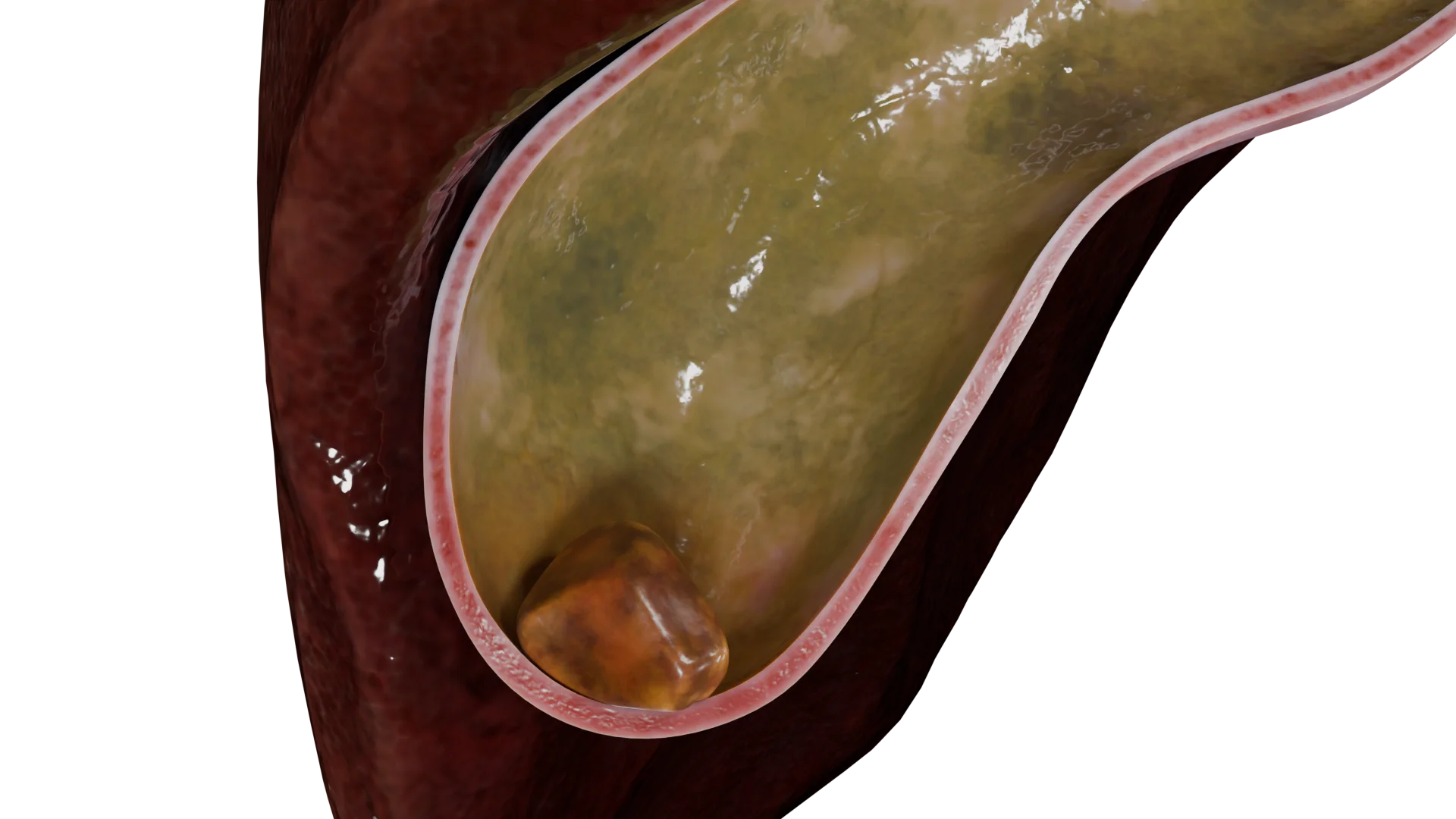
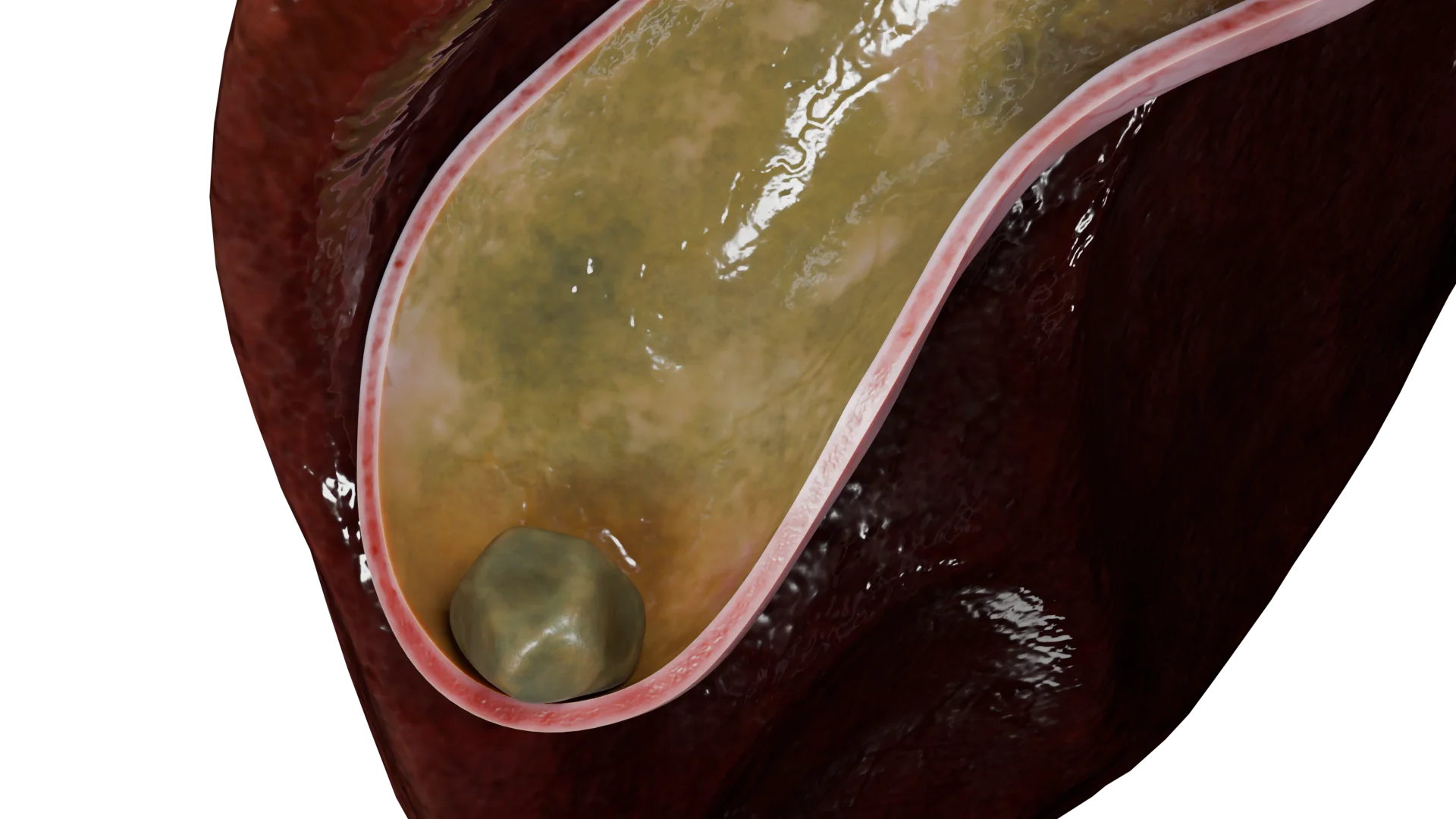
Acute calculous (catarrhal) cholecystitis – 3D Model
Classification of gallstone disease
The classification of gallstone disease includes the morphological characteristics, the number of calculi, and the clinical presentation of the disease.
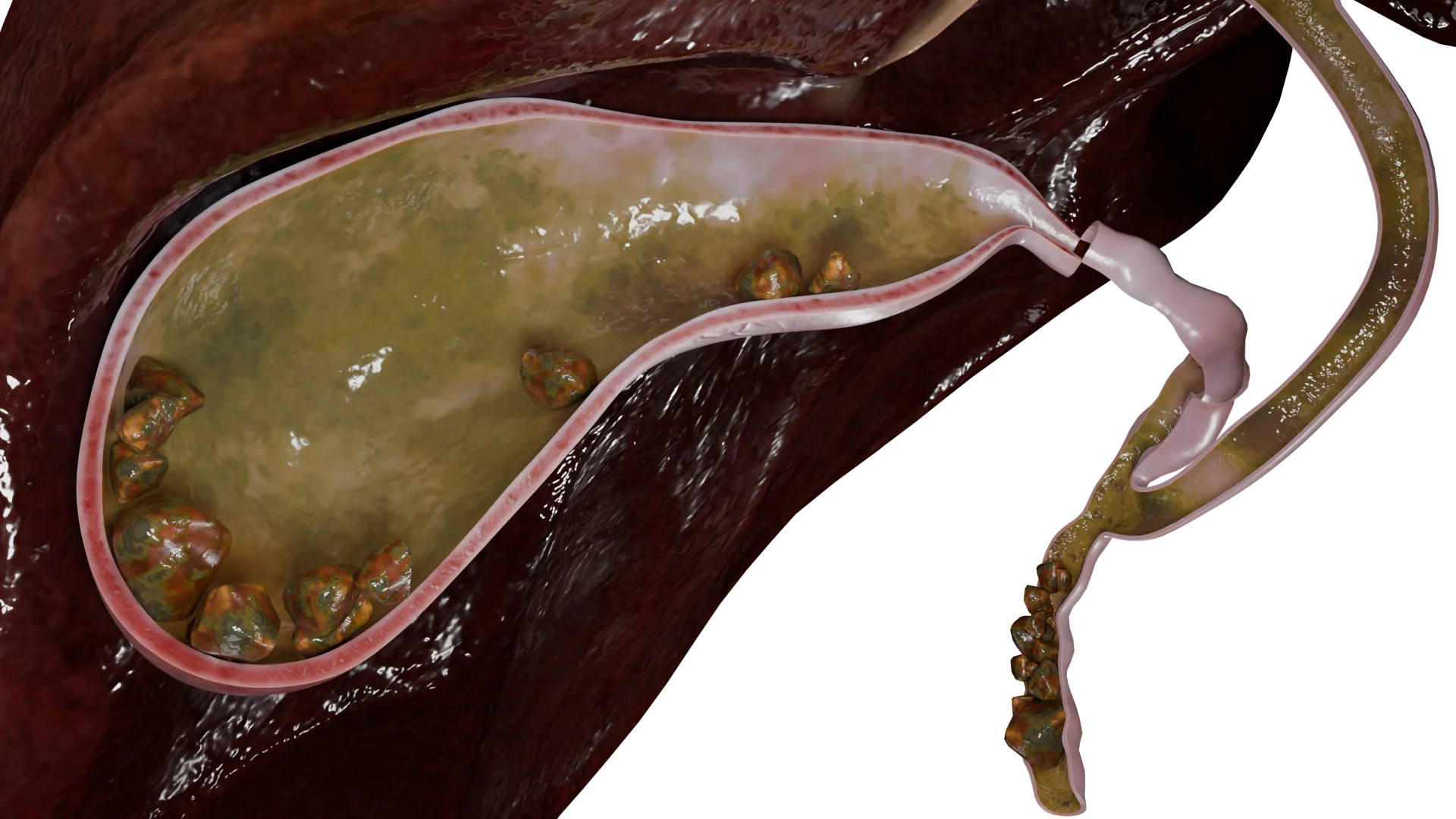
Single mixed calculus in the gallbladder without cholecystitis – 3D ModelMultiple mixed calculi in the gallbladder with acute cholecystitis – 3D-model
By clinical manifestations:
Asymptomatic gallstones;
With clinical signs and symptoms.
Clinical presentation
If a patient has no relevant complaints, cholelithiasis is considered asymptomatic.
Since there are no specific signs, gallstones in the hepatobiliary system are often an accidental finding during a routine abdominal examination.
The clinical manifestations of the disease include the following symptoms:
Pain syndrome;
Dyspeptic disorders;
(Frequently) jaundice;
Fever.
The pain syndrome is characterised by colicky pains that vary in intensity and duration. As a rule, the pain is associated with food intake, particularly the consumption of fatty meals. Colicky pain is usually localised in the right hypochondrium; sometimes the pain may radiate to the right lumbar and right groin areas.
An episode of biliary colic may resolve spontaneously without the need for antispasmodic therapy. During an attack, the patient may develop a low-grade or, in some cases, a high-grade fever.
Jaundice as a symptom develops when the biliary tract is obstructed by gallstones. The mechanism of obstruction is purely mechanical. Such patients typically present with yellowish discoloration of the skin, scleral icterus, dark urine and acholic (pale) stools.
Chronic cholecystitis and choledocholithiasis in the setting of gallstone disease: 3D Model
Dyspeptic manifestations are characterised by symptoms such as nausea, vomiting that does not bring relief, abdominal bloating, heartburn and decreased appetite.
Diagnosis of gallstone disease
Diagnosis of gallstone disease is based on physical examination, imaging and laboratory diagnostic methods.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of gallstone disease
Gallstone disease may be treated both with non-surgical therapy and surgical interventions.
Non-surgical therapy
Lifestyle modification is a key component in the treatment of gallstone disease:
Patients are advised to: avoid fatty, smoked and high-salt foods.
Elimination of unhealthy habits: including alcohol withdrawal and smoking cessation
Pharmacological therapy involves several groups of medications, depending on the therapeutic goal:
For pain relief: antispasmodic agents and nonsteroidal anti-inflammatory drugs (NSAIDs) are used;
Pathogenetic therapy: includes the use of ursodeoxycholic acid agents.
For the management of dyspeptic symptoms, prokinetic agents and proton pump inhibitors (PPIs) are prescribed;
During exacerbations: infusion therapy is administered for detoxification purposes.
As well, antibiotics are used to control infectious processes.
If conservative therapy appears ineffective, surgical intervention is indicated.
Surgical treatment
The main surgical procedures are aimed at removing the gallbladder or extracting stones from the bile ducts:
Cholecystectomy : removal of the gallbladder. It may be performed either as an elective or emergency procedure. Two primary surgical access types are used:
Laparoscopic cholecystectomy is performed through small incisions and considered the “gold standard” technique.
Open (laparotomic) cholecystectomy is performed through a conventional abdominal incision.
Choledocholithotomy: removal of stones from the common bile duct in cases where they have migrated from the gallbladder.
Sometimes, as part of an elective procedure, a patient may undergo a non-invasive treatment called lithotripsy that is the breaking up of stones using focused shock waves without any incisions. This method is used infrequently and is suitable only for certain types of gallstones.
FAQ
1. What are the causes and risk factors for the development of gallstone disease?
The primary causes of gallstone disease are bilirubin and cholesterol metabolism disorders, which lead to bile sludge and the formation of gallstones. Key risk factors include an imbalanced diet high in fats, low physical activity, female sex, advanced age, genetic predisposition, endocrine disorders, smoking, alcohol consumption, and impaired bile outflow.
2. How does gallstone disease manifest, and what are its symptoms?
Gallstone disease often remains asymptomatic (a condition known as silent stones). When clinical manifestations are present, the main symptom is an episode of pain in the right upper quadrant (biliary colic), which typically occurs after the consumption of fatty foods. Dyspeptic symptoms such as nausea, vomiting, bloating and heartburn may also be observed.
3. What are the potential complications and risks of gallstone disease?
The major danger and primary complication is mechanical obstruction of the biliary tract by a gallstone. This condition can lead to severe attacks of biliary colic, fever and obstructive jaundice, characterised by yellowing of the skin, dark urine, and pale (acholic) stools.
4. What diet and nutritional recommendations are advised for patients with gallstone disease, and which foods should be avoided?
Diet is an essential component of the non-surgical therapy. It is recommended to exclude fatty, smoked, and salty foods from the diet. Patients should also avoid alcohol consumption and smoking, as these factors can trigger exacerbations of the disease.
5. How to relieve an episode of biliary colic in gallstone disease?
An acute attack of biliary colic is relieved with pharmacological therapy. Antispasmodic agents are administered to relieve smooth muscle spasm of the biliary tract, while nonsteroidal anti-inflammatory drugs (NSAIDs) are used to reduce pain and inflammation. During exacerbations, infusion therapy may be administered for detoxification and supportive care.
6. Is it possible to treat gallstone disease without surgery?
Yes. Non-surgical (conservative) treatment is the primary approach when there are no indications for emergency surgery. It includes several therapeutic approaches. The main pathogenetic treatment involves the use of ursodeoxycholic acid (UDCA) agents, which, when administered over a prolonged period, can dissolve cholesterol gallstones. In selected cases, a noninvasive procedure called lithotripsy (stone fragmentation using focused shock waves) may also be applied. An essential component of such a treatment is adherence to a strict diet.
7. What are the indications for surgical intervention in gallstone disease?
Surgical treatment, including gallbladder removal (cholecystectomy), is indicated when non-surgical therapy appears ineffective and biliary colic episodes cannot be relieved and occur despite the therapy. The procedure may be performed either electively or on an emergency basis.
8. Is there a way to prevent gallstone disease?
Prevention focuses on minimising risk factors. Preventive measures include maintaining a healthy diet, regular physical activity, controlling body weight and comorbid conditions and avoiding bad habits.
9. Can gallstone disease occur in children?
Yes, gallstone disease can occur in children, although it is significantly less common than in adults. Unlike in adults, the main risk factors in children are often not related to lifestyle but to underlying medical conditions such as haemolytic anaemias (for example, sickle cell anemia), prolonged parenteral nutrition, prematurity, cystic fibrosis and congenital abnormalities of the biliary tract. Clinical presentation in pediatric patients may be atypical, ranging from abdominal pain and nausea to completely asymptomatic cases. Treatment depends on the presence of symptoms: in asymptomatic cases, a watchful waiting approach may be appropriate, whereas in symptomatic patients, the main method of treatment — as in adults — is gallbladder removal (cholecystectomy).
References
1.
VOKA Catalogue. [Electronic resource].
https://catalog.voka.io/
2.
Дадвани С.А., Ветшев П.С., Шулутко A.M., Прудков М.И. Желчнокаменная болезнь. М.: Видар, 2000. 144 с.
3.
Дорофеева, С.Г., Конопля, Е.Н., Мансимова, О.В., Шелухина, А.Н., Анюшонков, О.С. Желчнокаменная болезнь: современные представления об этиологии и патогенезе. Интегративные тенденции в медицине и образовании, 2020. Vol. 2 C. 21-25.
4.
Ивашкин В.Т., Маев И.В., Баранская Е.К. Рекомендации Российской гастроэнтерологической ассоциации по диагностике и лечению желчнокаменной болезни. РЖГГК, 2016. 3: 64-80.(Савельев B.C., Кириенко А.И. Хирургические болезни. Том 1. М.: 2005. С. 185-201.) [in Russian].
5.
EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. Journal of Hepatology. 2016. 65: 146–181.
6.
Лейшнер У. Практическое руководство по заболеваниям желчных путей. Moscow: GEOTAR – Medicine; 2001, 264 p. (Лейшнер У. Практическое руководство по заболеваниям желчных путей. М.: ГЭОТАР – Медицина, 2001. 264с.) [in Russian]
7.
Литовский И.А., Гордиенко А.В. Желчнокаменная болезнь, холециститы и некоторые ассоциированные с ними заболевания (вопросы патогенеза, диагностики, лечения). Санкт-Петербург: СпецЛит, 2019. 358 с.
8.
Podoluzhnyi V.I. Complications of gallstone disease. Fundamental and Clinical Medicine. 2017; Vol. 2(1). 102-114. (Подолужный В.И. Осложнения желчнокаменной болезни. Фундаментальная и клиническая медицина. 2017;2(1):102-114) [in Russian]
9.
Savelyev, V. S., Kirienko, A. I. Surgical Diseases Vol. 1 Moscow: 2005. 185-201.(Савельев B.C., Кириенко А.И. Хирургические болезни. Том 1. М.: 2005. С. 185-201.) [in Russian].
10.
Скворцов, В.В., Халилова, У.А. Диагностика и лечение желчнокаменной болезни. Экспериментальная и клиническая гастроэнтерология, 2018. Том 157. № 9. 142-150. (Подолужный В.И. Осложнения желчнокаменной болезни. Фундаментальная и клиническая медицина. 2017;2(1):102-114) [in Russian]
11.
Успенский, Ю.П., Фоминых, Ю.А., Наджафова, К.Н. Липидный обмен у лиц с желчнокаменной болезнью. University Therapeutic Journal, 2020. Том 2. № 1. 74-75. (Подолужный В.И. Осложнения желчнокаменной болезни. Фундаментальная и клиническая медицина. 2017;2(1):102-114) [in Russian]
12.
Khimich, S.D. Analysis of Morphofunctional Features of the Development and Course of Certain Acute Surgical Diseases of the Abdominal Organs in Patients with Obesity: abstract of Dissertation for the Degree of Doctor of Medical Sciences. [in Russian] – М., 2002. 38p. (Химич С.Д. Анализ морфо-функциональных особенностей развития и течения некоторых острых хирургических заболеваний органов брюшной полости у лиц с ожирением: автореферат диссертации на соискание ученой степени докт. мед. наук. – М., 2002, 38с.) [in Russian]
13.
Barak O., Elazary R., Appelbaum L., Rivkind A., Almogy G. Conservative treatment for acute cholecystitis: clinical and radiographic predictors of failure. Isr Med Assoc J, 2009; 11: 739–743.
Cotton P.B., Elta G.H., Carter C.R., Pasricha P.J., Corazziari E.S. Rome IV. Gallbladder and Sphincter of Oddi Disorders. Gastroenterology, 2016 Feb 19. pii: S0016-5085(16)00224-9.
16.
McGlone E.R., Bloom S.R. Bile acids and the metabolic syndrome. Annals of Clinical Biochemistry, 2019, т. 56, № 3, p. 326–337.
17.
Wang Y., Qi M., Qin C., Hong J. Role of the biliary microbiome in gallstone disease. Expert Review of Gastroenterology & Hepatology, 2018, T 12, № 12, p. 1193–1205.