Cholecystitis: Etiology, Classification, Clinical Manifestations, Diagnosis, and Treatment
Aleksandr F.Abdominal surgeon, MD
10 min read·October 30, 2025
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Cholecystitis is an inflammation in the gallbladder caused by impaired bile outflow. The condition may develop due to a mechanical obstruction by gallstones (calculous cholecystitis) or for other reasons (acalculous cholecystitis).
Classification of Cholecystitis
By type of the disease:
Acute,
Chronic.
Acute Catarrhal Cholecystitis Associated with Gallstones — 3D ModelChronic Cholecystitis Associated with Gallstones, without Acute Exacerbation — 3D Model
By etiology:
Calculous (associated with gallstones),
Acalculous (not caused by gallstones).
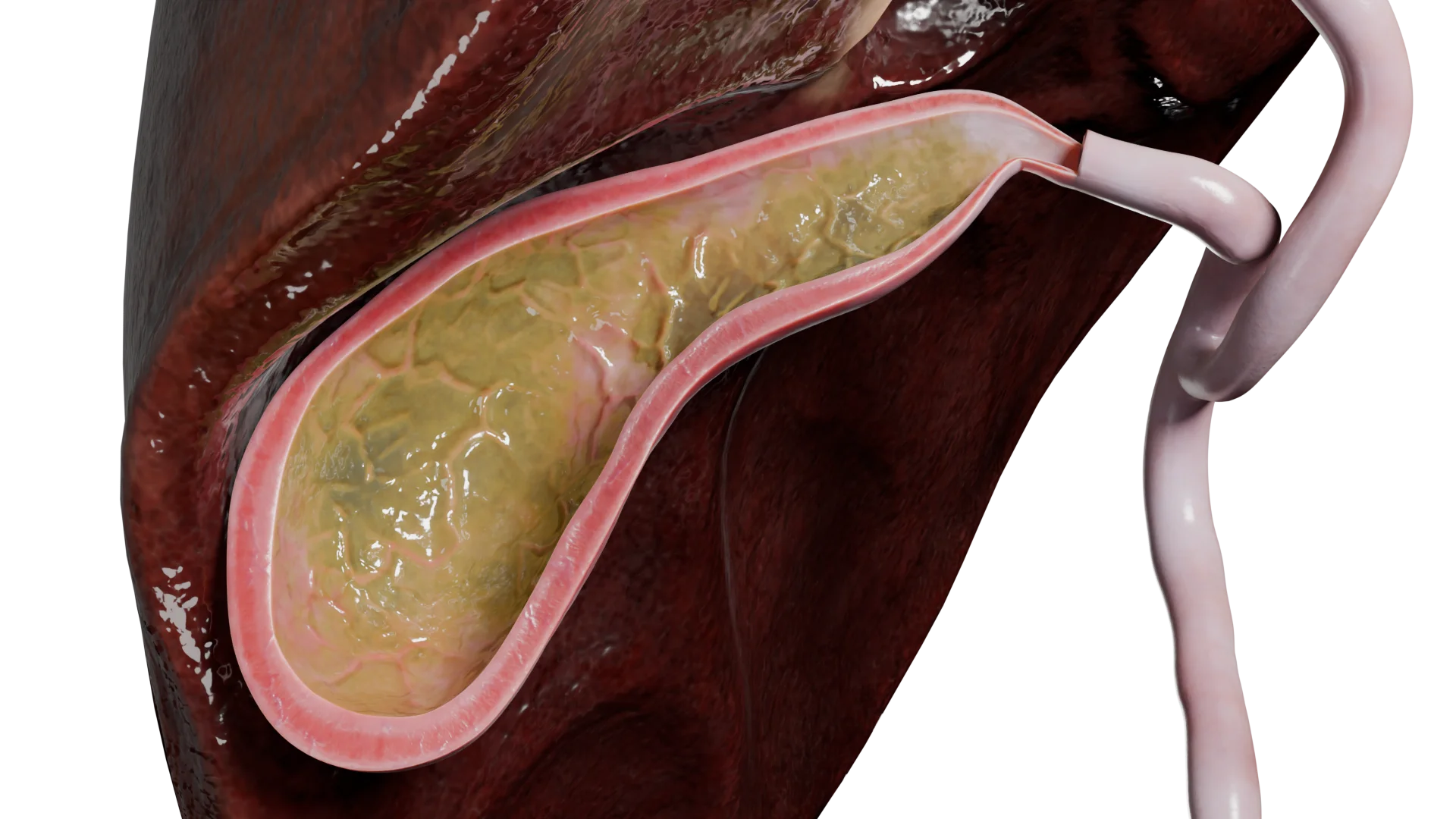
Acute Calculous Catarrhal Cholecystitis — 3D ModelAcute Catarrhal Cholecystitis without Gallstones — 3D Model
By clinical and morphological features:
Catarrhal,
Phlegmonous,
Gangrenous.
3D models of cholecystitis according to clinical and morphological features:
Acute Catarrhal Cholecystitis
Acute Phlegmonous Cholecystitis
Acute Gangrenous Cholecystitis
By severity:
Mild: limited gallbladder inflammation;
Moderate: gallbladder inflammation persists for more than 72 hours, and its walls bear signs of destructive changes;
Severe: total gallbladder destruction accompanied by signs of multiple organ failure.
Etiology and Pathogenesis
Inflammation of the gallbladder wall may arise due to certain damaging factors.
Based on the cause, cholecystitis is differentiated into its calculous and acalculous forms.
Calculous cholecystitis
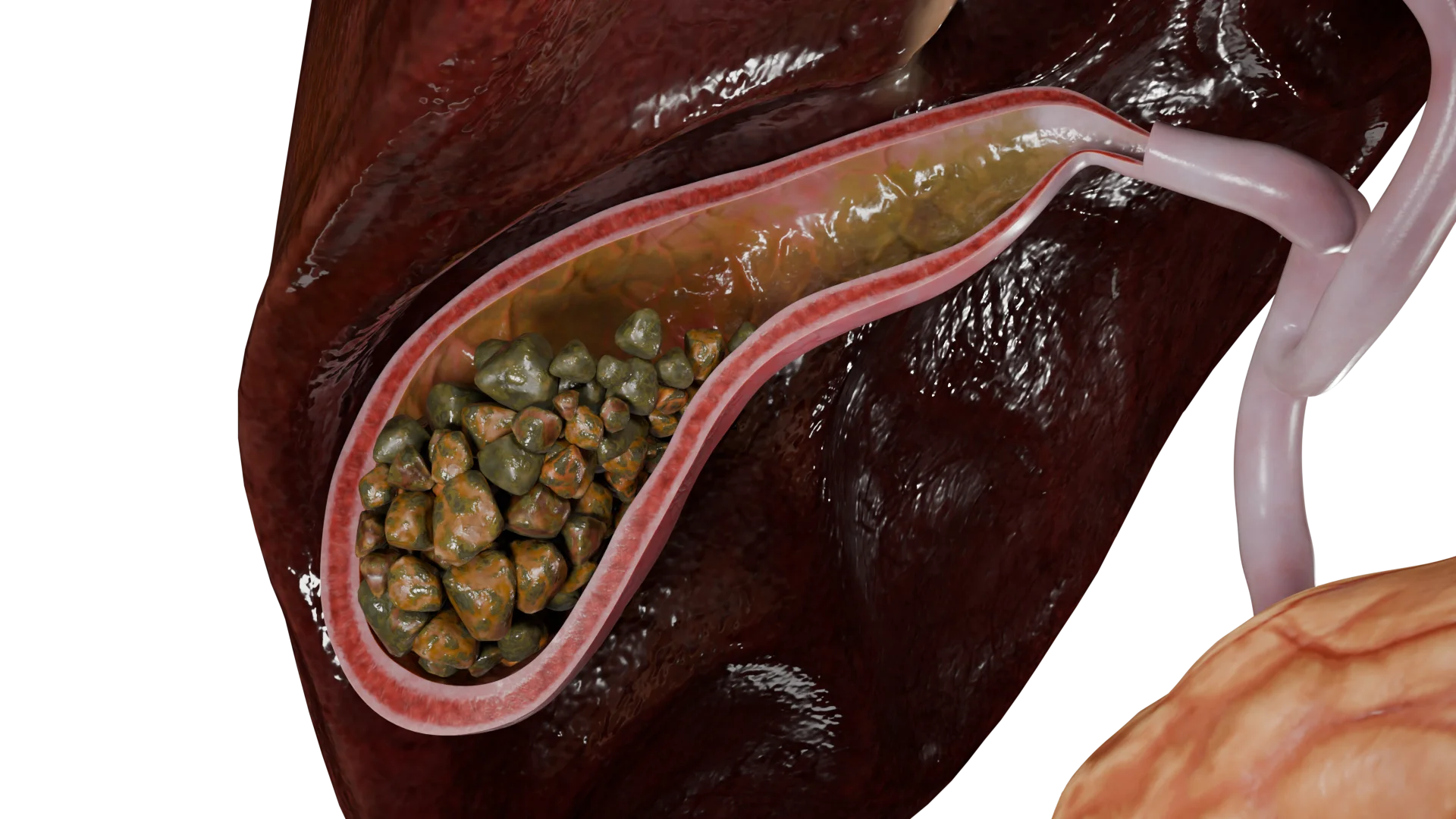
Calculouscholecystitis develops secondary to gallstones (cholelithiasis) when a solitary or multiple calculi obstruct the cystic duct or gallbladder neck. The obstruction increases intraluminal gallbladder pressure, damages its mucosa, and causes local ischemic changes in the gallbladder wall. This triggers inflammation and the release of biologically active substances and inflammatory mediators.
Multiple Gallstones in Gallbladder and Cystic Duct — 3D Model
Only 50–75% of cholecystitis cases secondary to cholelithiasis have a bacterial nature. The most commonly identified gram-negative bacteria are: E. coli, Klebsiella spp., Pseudomonas spp., Enterobacter spp. Among gram-positive bacteria, Enterococcus spp. and Streptococcus spp. are most frequent. Anaerobes include Clostridium spp.
Acalculous cholecystitis
Unlike the calculous form,acalculous cholecystitis is caused by a variety of factors, such as impaired gallbladder contractility, hematogenous infection, systemic conditions, intestinal infections, or congenital bile duct disorders (e.g., choledochal cyst). However, all of these causes follow the same inflammation mechanism in the gallbladder wall that is typically observed in calculous cholecystitis.
Clinical Manifestations
Cholecystitis is associated with a range of signs and symptoms, such as:
Pain,
Dyspepsia,
Inflammation,
Peritoneal irritation,
Obstructive jaundice.
In general, pain in cholecystitis typically manifests as biliary colic. The episode of biliary colic may resolve spontaneously or with the help of antispasmodic drugs. The pain is intense. It is typically localized in the right upper quadrant (right hypochondrium) but may sometimes radiate to the adjacent regions (lumbar region, scapula, or shoulder). As the condition progresses, the pain tends to exacerbate and irritate the peritoneum.
Furthermore, dyspepsia may develop secondary to pain. This syndrome covers nausea, vomiting, and a bitter taste in the mouth. Vomiting, either single-episode or repeated, usually brings no relief.
Even during the first few days, patients often have a low-grade fever, which may gradually rise to a moderate fever as the inflammation progresses.
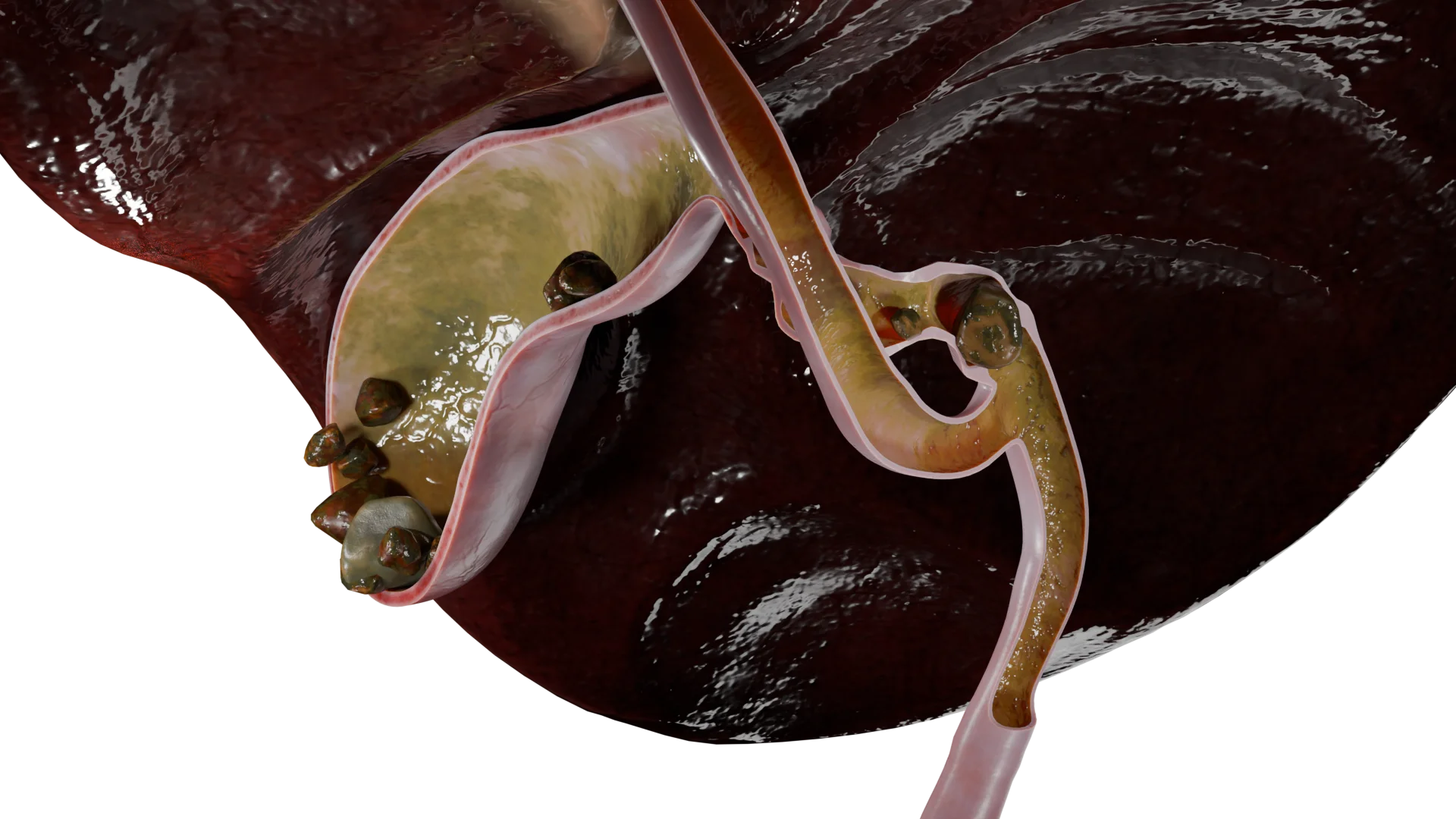
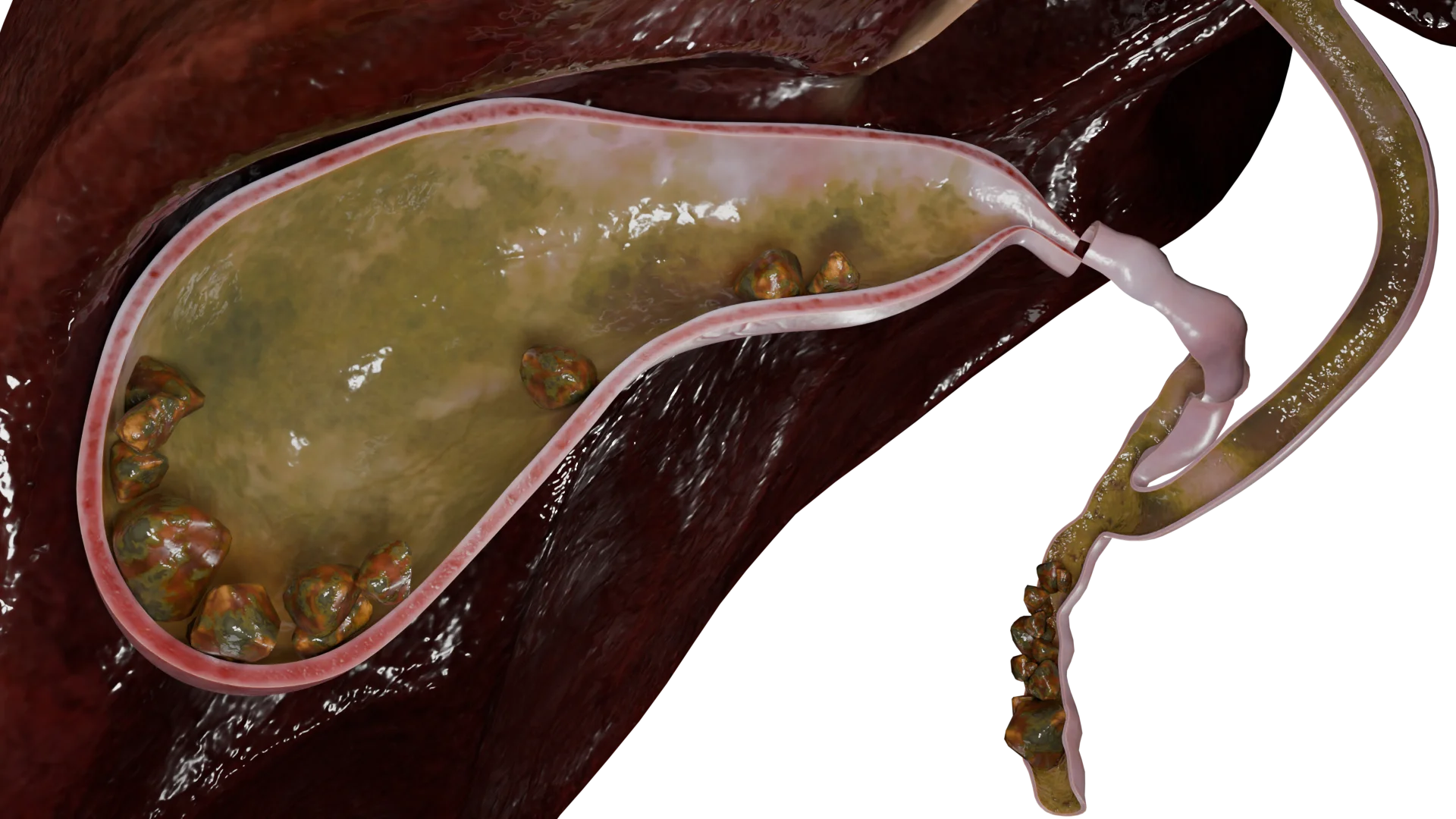
During examination, a healthcare professional should pay particular attention to signs of jaundice, including the yellow discoloration of the skin, sclerae, and mucous membranes. Dark urine and pale stools are quite common. The primary cause of these symptoms is a gallstone, either solitary or multiple, that obstructs (or blocks) the hepatobiliary system.
Multiple Gallstones in Gallbladder and Bile Duct — 3D Model
Diagnosis of Cholecystitis
Diagnosis of cholecystitis is based on clinical evaluation and investigations (both laboratory and instrumental).
Laboratory tests: complete blood count (CBC), urinalysis, and blood tests (liver function tests, inflammatory markers, electrolytes). In critically ill patients, the acid-base balance should also be assessed.
Investigations: abdominal ultrasound, plain abdominal and chest X-ray, computed tomography (CT), and esophagogastroduodenoscopy (EGD).
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Treatment of Cholecystitis
Cholecystitis can be managed with medical or surgical approaches.
Medical Management
Medical therapy is aimed at stabilizing the acute episode and preparing the patient for potential surgery.
Pain relief: Nonsteroidal anti-inflammatory drugs (NSAIDs) and antispasmodics are used to control pain.
Infusion therapy: Intravenous fluids help to reverse any toxic effects of the condition and restore fluid and electrolyte balance.
Antimicrobial therapy: Antibiotics are administered when signs of a bacterial infection develop. The exact medications are chosen based on microbial sensitivity and the patient’s allergy history.
Surgical Management
Surgical removal of the gallbladder (cholecystectomy) is the definitive treatment for cholecystitis.
If conservative treatment has proven efficient and acute cholecystitis has no complications, elective cholecystectomy may be performed. However, when medications have failed and the condition progresses, emergency surgery is required. In this case, the intervention is most feasible within the first 24–72 hours after the onset.
There are two main surgical approaches:
Laparoscopic cholecystectomy: Removal of the gallbladder through small abdominal incisions; minimally invasive and considered the gold standard.
Open cholecystectomy: Performed through either an upper midline incision or an incision in the right hypochondriac region.
FAQ
1. What are calculous and acalculous cholecystitis, and what causes them?
Cholecystitis is an inflammation of the gallbladder. The most common type is calculous cholecystitis, which occurs secondary to gallstones. When these stones block the cystic duct, they can trigger an acute episode. In chronic cases, gallstones may be present without causing any obstruction. Acalculous cholecystitis is less common and is not related to gallstones. It often results from poor gallbladder motility, severe infections, or circulatory disorders.
2. What are the symptoms of cholecystitis, and how does an acute episode present?
One of the main symptoms is sudden, intense pain in the right upper quadrant (right hypochondrium), commonly known as biliary colic. The pain may be accompanied by nausea, vomiting, fever, and a bitter taste in the mouth. Chronic cholecystitis can flare up with similar symptoms, though they are usually milder. If bile flow becomes obstructed, jaundice may develop, along with dark urine and pale stools.
3. What complications can arise from cholecystitis, and why is it dangerous?
If left untreated, cholecystitis can lead to serious complications. The inflammation may progress to destructive forms, such as phlegmonous or gangrenous cholecystitis, which can cause gallbladder wall perforation and peritonitis. In severe cases, it can result in multiple organ failure and become life-threatening.
4. How is cholecystitis treated, and can it be cured permanently?
According to modern clinical practice, treatment usually begins with conservative therapy to relieve acute symptoms. This may include painkillers, antispasmodics, and antibiotics if a bacterial infection is suspected. However, the only definitive way to cure calculous cholecystitis and prevent recurrence and complications is surgical removal of the gallbladder (cholecystectomy).
5. What laboratory and imaging tests are used to diagnose cholecystitis?
Diagnosis combines laboratory tests and imaging studies. Abdominal ultrasound is considered the gold standard and can reveal gallbladder wall thickening, gallstones, and other typical signs of inflammation. In more complex or unclear cases, CT scans may be performed to provide a more detailed assessment.
6. Can an episode of cholecystitis resolve without treatment?
The pain of biliary colic may subside on its own, but this does not mean the inflammation has resolved. The underlying disease process usually persists, and without proper treatment, it may progress, increasing the risk of serious complications.
7. What diet is recommended for acute and chronic cholecystitis?
Diet plays a key role in treatment. During an acute episode, fasting is usually recommended first, followed by a strict therapeutic diet that excludes fatty, fried, spicy foods and alcohol. In chronic cholecystitis during remission, similar dietary principles apply but can be followed with greater flexibility. Meals should be small and frequent, ideally 5–6 times a day.
8. How does cholecystitis differ from cholestasis?
These are different conditions. Cholecystitis is inflammation of the gallbladder wall. Cholestasis, on the other hand, refers to a reduced or blocked bile flow from the liver. It can contribute to gallbladder inflammation, but it is not the same condition.
9. Can cholecystitis be prevented?
Yes. Preventive measures focus on reducing the risk of gallstone formation. A balanced diet low in fat and rich in fiber, maintaining a healthy weight, regular physical activity, and adequate hydration can help lower the risk of developing the disease.
10. How does cholecystitis present in children?
Cholecystitis is uncommon in children and is usually acalculous. It may develop as a complication after severe infections (such as scarlet fever or sepsis) or as part of systemic diseases. Symptoms are generally similar to those in adults. Treatment is based on antibiotic therapy and, when required, surgical intervention.
Dorofeeva, S. G., Konoplya, E. N., Mansimova, O. V., Shelukhina, A. N., & Anyushonkov, O. S. (2020). Zhelchnokamennaya bolezn: sovremennye predstavleniya ob etiologii i patogeneze [Gallstone disease: Modern views on etiology and pathogenesis]. Integrativnye tendentsii v meditsine i obrazovanii, 2, 21–25.
4.
Ivashkin V.T., Maev I.V., Baranskaya E.K.
Recommendations of the Russian Gastroenterological Association for the diagnosis and treatment of gallstone disease. Russian Journal of Gastroenterology, Hepatology, Coloproctology. 2016;3:64–80. (Ивашкин В.Т., Маев И.В., Баранская Е.К. Рекомендации Российской гастроэнтерологической ассоциации по диагностике и лечению желчнокаменной болезни. РЖГГК, 2016. Т.3. С. 64-80.) [in Russian]
5.
EASL Clinical Practice Guidelines on the prevention, diagnosis and treatment of gallstones. Journal of Hepatology, 2016. 65: 146–181.
6.
Leuschner U. Practical Guide to Biliary Tract Diseases. Moscow: GEOTAR – Medicine; 2001, 264 p. (Лейшнер У. Практическое руководство по заболеваниям желчных путей. М.: ГЭОТАР – Медицина, 2001. 264с.) 264 с.
7.
Litovskiy, I. A., & Gordienko, A. V. (2019). Zhelchnokamennaya bolezn, kholecistity i nekotorye assotsiirovannye s nimi zabolevaniya: Voprosy patogeneza, diagnostiki, lecheniya [Gallstone disease, cholecystitis, and some associated diseases: Pathogenesis, diagnosis, treatment]. SpetsLit. 358 p.
8.
Podoluzhnyi V.I. Complications of gallstone disease. Fundamental and Clinical Medicine. 2017; Vol. 2(1). 102-114. (Подолужный В.И. Осложнения желчнокаменной болезни. Фундаментальная и клиническая медицина. 2017;2(1):102-114) [in Russian]
9.
Savelyev, V. S., Kirienko, A. I. Surgical Diseases Moscow: 2005. V. 1. 185-201.(Савельев B.C., Кириенко А.И. Хирургические болезни. Том 1. М.: 2005. С. 185-201.) [in Russian].
10.
Skvortsov V.V., Khalilova U.A. Diagnosis and treatment of gallstone disease. Experimental and clinical gastroenterology. 2018; Vol. 157, No. 9, p. 142–150 (Скворцов, В.В., Халилова, У.А. Диагностика и лечение желчнокаменной болезни. Экспериментальная и клиническая гастроэнтерология, 2018. Том 157. № 9. C. 142–150.) [in Russian]
11.
Uspensky, Y.P., Fominykh, Y.A., Nadzhafova, K.N. (2020). Lipid metabolism in patients with gallstone disease. University Therapeutic Journal, 2(1), 74–75. (Успенский, Ю.П., Фоминых, Ю.А., Наджафова, К.Н. Липидный обмен у лиц с желчнокаменной болезнью. University Therapeutic Journal, 2020. Том 2. № 1. C. 74–75.) [in Russian]
12.
Khimich, S.D. Analysis of Morphofunctional Features of the Development and Course of Certain Acute Surgical Diseases of the Abdominal Organs in Patients with Obesity: abstract of Dissertation for the Degree of Doctor of Medical Sciences. [in Russian] 38 p. 38 с.
13.
Barak O., Elazary R., Appelbaum L., Rivkind A., Almogy G. Conservative treatment for acute cholecystitis: clinical and radiographic predictors of failure. Israel Medical Association Journal, 11, 11. 739–743.
14.
Chen, L. Y., Qiao, Q. H., Zhang, S. C., Chen, Y. H., Chao, G. Q., & Fang, L. Z. (2012). Metabolic syndrome and gallstone disease. World Journal of Gastroenterology, 18, 4215–4220.
15.
Cotton P.B., Elta G.H., Carter C.R., Pasricha P.J., Corazziari E.S. Rome IV. Gallbladder and Sphincter of Oddi Disorders. Gastroenterology, pii: S0016-5085(16)00224-9.
16.
McGlone E.R., Bloom S.R. Bile acids and the metabolic syndrome. Annals of Clinical Biochemistry, 56(3), 56(3). 326–337.
17.
Wang Y., Qi M., Qin C., Hong J. Role of the biliary microbiome in gallstone disease. Expert Review of Gastroenterology & Hepatology, 12(12), 12(12). 1193–1205.