Skin Biopsy in Dermatology: Classification, Technique, and Diagnostic Value
Polina S.Dermatologist, MD
9 min read·January 29, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
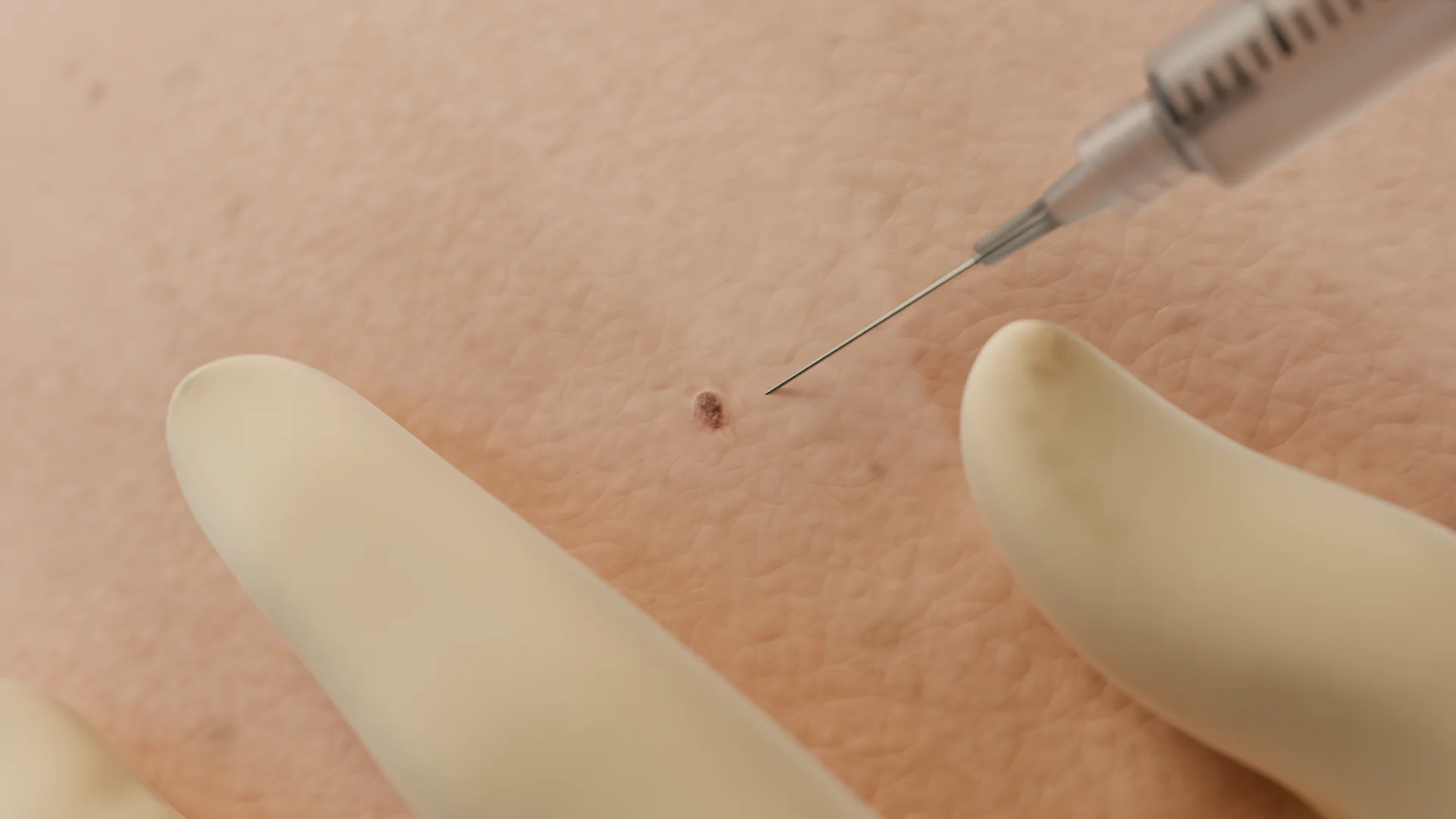
A skin biopsy is an invasive diagnostic procedure in which a small tissue sample is removed for morphological evaluation. Depending on the clinical question, the specimen may include the epidermis, the dermis, and, when needed, subcutaneous fat. Skin biopsy provides a high diagnostic yield and, in some cases, remains the only way to establish a definitive diagnosis.
Microscopic examination of the biopsy specimen provides detailed information about cellular and tissue architecture, the presence of a pathologic process, the nature of a tumor, and the extent of tissue changes. In clinical practice, biopsy supports early diagnosis and helps guide timely management, reducing the risk of complications.
3D Animation: Skin Biopsy
History and Development of PRP Therapy
Early descriptions of skin biopsy date to the 19th century, when microscopy began to be used to support and confirm clinical diagnoses.
In the 20th century, standardized biopsy techniques made specimen collection faster and more reproducible. Today, advances in histopathology and molecular diagnostics make it possible to obtain highly accurate results while minimizing tissue trauma.
Clinical Purpose and Indications for Skin Biopsy
Diagnostic confirmation: to confirm or refine a clinical diagnosis.
Differential diagnosis: to distinguish between clinically similar dermatoses.
Cancer detection: to identify malignant and premalignant condition.
Staging and activity assessment: to evaluate disease stage and activity.
Treatment monitoring: to assess response to therapy.
Classification
In current dermatologic practice, skin biopsy can be classified in several ways.
By the amount of tissue removed
Excisional skin biopsy: complete removal of a lesion, typically with a margin of clinically normal tissue.
Incisional skin biopsy: removal of a portion of a lesion within the pathologic focus.
In most cases, no special preparation is required. The procedure typically takes 15 to 20 minutes and is performed in a procedure room or operating room. Before sampling, the clinician performs antiseptic skin preparation and administers local anesthesia. The biopsy technique is selected based on the lesion’s morphology, size, and anatomic location.
Antiseptic skin preparation
Local anesthesia
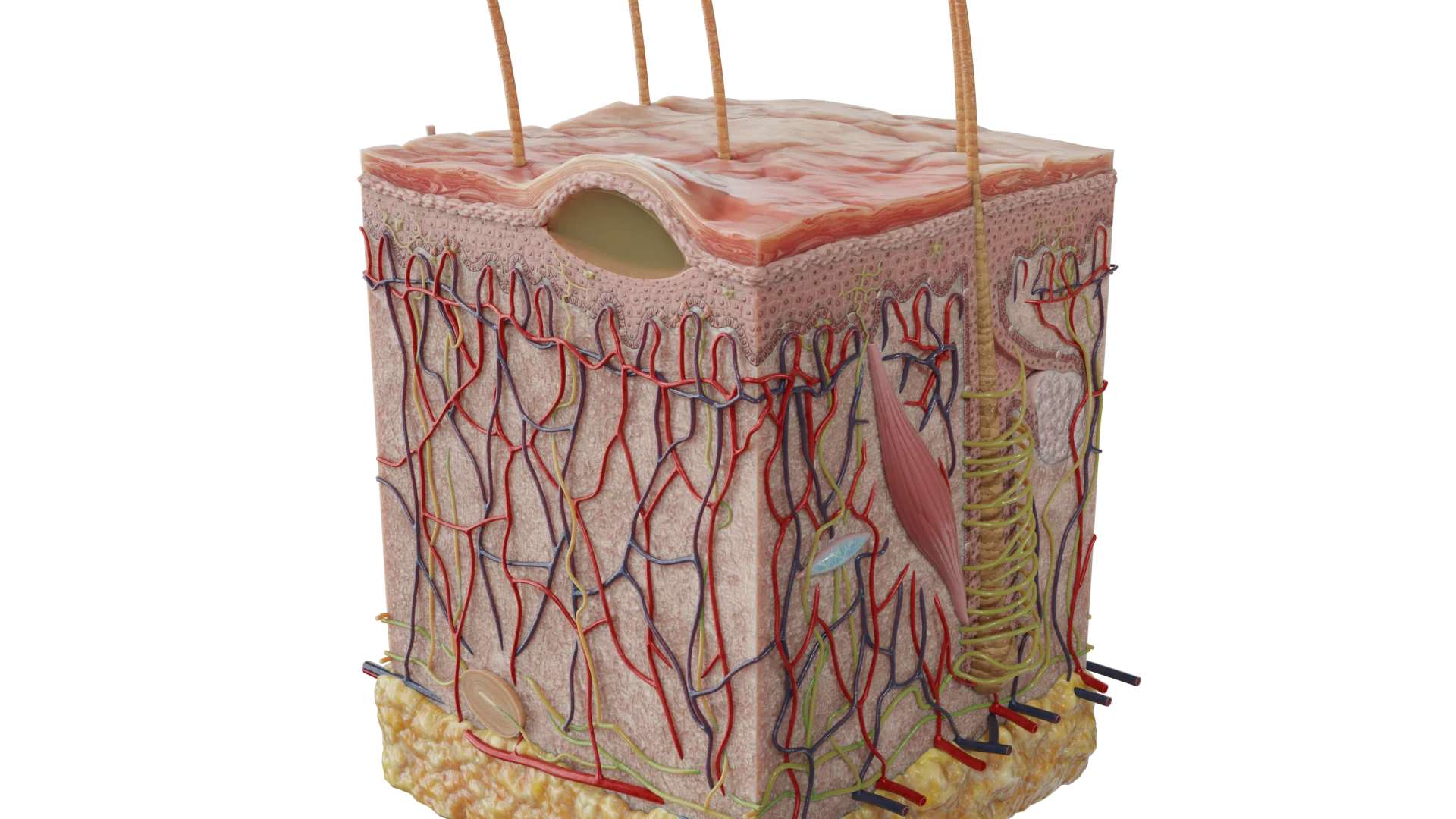
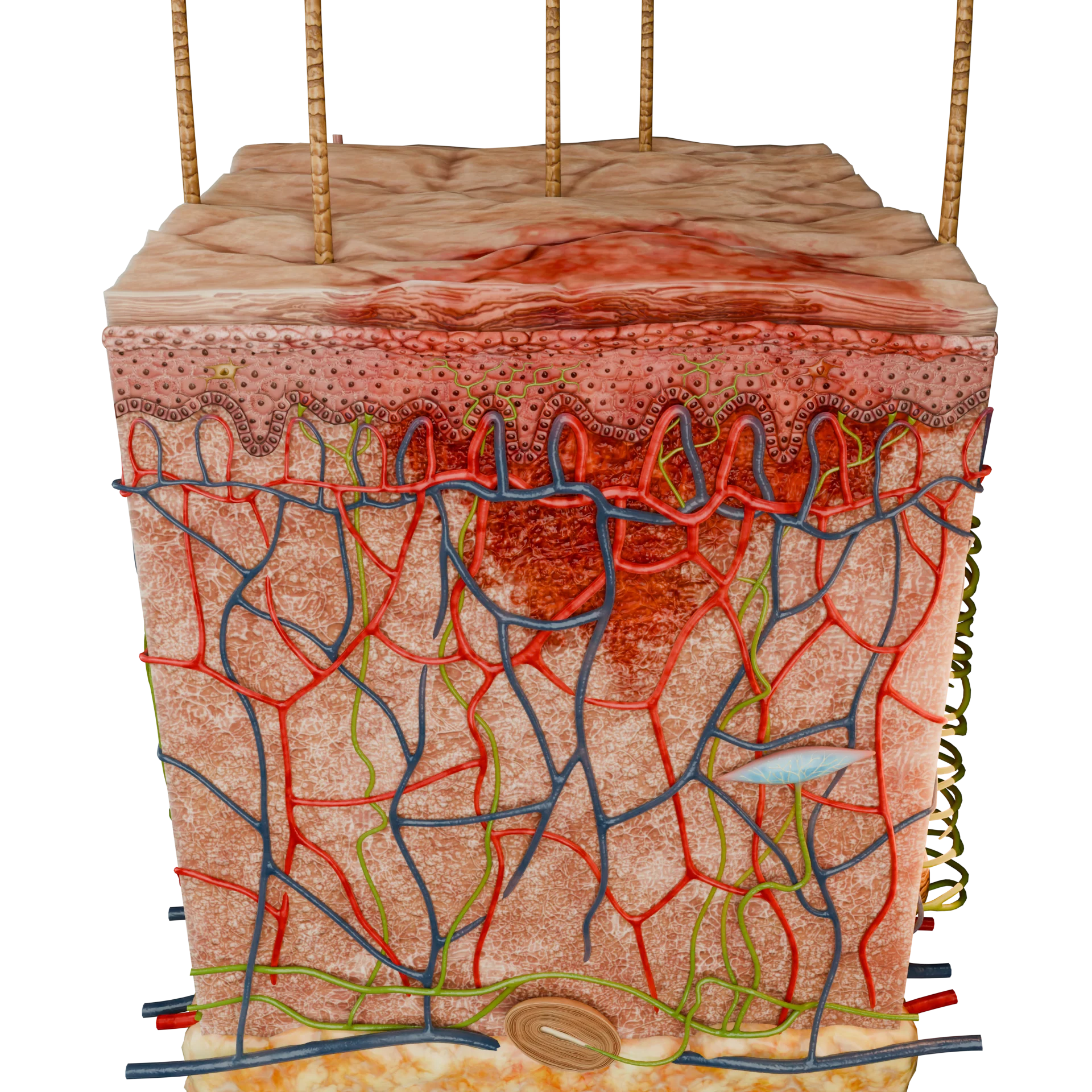
Biopsy depth should match the suspected diagnosis and the goals of histologic evaluation. For superficial inflammatory processes, sampling may be limited to the dermis. For deep infiltrative processes, the specimen should include subcutaneous fat, as key diagnostic changes may be present below the dermis.
Punch Biopsy
Rotating the biopsy punch
Grasping and removing the specimen
A sterile, single-use biopsy punch is positioned perpendicular to the skin surface and advanced with a rotating motion to the level of the subcutaneous fat. The tissue cylinder is gently lifted with forceps and transected at the base using scissors or a scalpel. If needed, one or two interrupted sutures are placed. The site is then covered with a sterile dressing.
Punch biopsy is widely used for inflammatory, non-neoplastic skin disorders and for evaluation of vasculitis. It allows sampling across skin layers with minimal tissue disruption when performed correctly.
Shave Biopsy (Superficial Shave, Razor Technique)
Removing the lesion with a specialized blade
The lesion is removed parallel to the skin surface using a disposable razor or blade. The sample is superficial and typically does not include the deep dermis. Sutures are usually unnecessary, and the wound is covered with a sterile dressing.
Shave biopsy is most often used for pedunculated lesions, papules, and other raised growths, including seborrheic keratoses and warts. For most inflammatory dermatoses, this technique is less informative because it may not capture the depth needed for diagnosis.
Excisional Skin Biopsy
Wide excision of the lesion with a scalpel
After antiseptic skin preparation and local anesthesia, an elliptical incision is made with a scalpel. The lesion is removed in full thickness, including subcutaneous fat, with margins extending into clinically normal tissue when appropriate for diagnostic evaluation. After hemostasis is achieved, the wound is closed with simple interrupted or subcuticular sutures, and a sterile dressing is applied.
Excisional biopsy is indicated when benign or malignant neoplasms are suspected, including papillomas, warts, seborrheic and actinic keratoses, pyogenic granulomas, and rhinophyma. It may also be used to remove hypertrophic scars or scars of cosmetic concern.
Specimen Handling, Fixation, and Transport
Placing the specimen in fixative
Histopathologic evaluation
Immediately after sampling, the specimen is placed in a fixative, most commonly 10% neutral buffered formalin. The pathology request form should include essential clinical details, such as lesion location, duration, clinical appearance, relevant history, and the clinician’s differential diagnosis. Clear clinical context improves the accuracy and clinical relevance of the pathologist’s report.
Depending on the clinical indication, the specimen may be submitted for:
Histological examination;
Immunohistochemistry (IHC);
Direct and indirect immunofluorescence (DIF/IIF);
Molecular genetic testing.
Indications for Skin Biopsy
Suspected malignant skin neoplasms;
Inflammatory dermatoses of unclear etiology;
Bullous disorders and autoimmune skin diseases;
Chronic ulcers and infiltrative lesions;
Skin infections with atypical presentation or course.
Contraindications
Severe coagulation disorders,
Acute purulent infection at the planned biopsy site,
Severe overall patient condition that makes the procedure unsafe.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Complications and Limitations
Complications after skin biopsy are rare. When they do occur, pain is the most common. Bleeding, keloid formation, and infection are less frequent.
Although skin biopsy is highly valuable, it has practical limitations and requires clinical expertise. An incorrect method, suboptimal site selection, or insufficient depth can result in a non-diagnostic specimen.
FAQ
1. What is a skin biopsy, and why is it performed?
A skin biopsy is an invasive diagnostic procedure in which a small tissue sample is removed for morphologic evaluation. Depending on the clinical question, the specimen may include the epidermis, the dermis, and, when needed, subcutaneous fat. The procedure is used when a clinical (visual) exam is not sufficient to establish an accurate diagnosis. It is especially important when malignancy or premalignancy is suspected, as well as in cases of dermatoses that remain unclear after examination.
2. What does a skin biopsy feel like?
Because the procedure is performed with local anesthesia, most patients feel little to no pain during the biopsy itself. You may notice a brief sting at the moment the anesthetic is injected. After the anesthetic effect subsides, the area may feel tender, and mild to moderate discomfort at the site is possible.
3. How is a skin biopsy taken?
The procedure is performed after antiseptic skin preparation and local anesthesia. The sampling method depends on the clinical goal. For example, a punch biopsy uses a rotating punch instrument, a shave biopsy uses a blade to remove a superficial sample, and an excisional biopsy is performed with a scalpel.
4. Why might a biopsy be ordered for psoriasis or atopic dermatitis?
Although these conditions often have characteristic clinical features, a biopsy may be needed when the presentation is atypical. In that situation, microscopic evaluation can support a more accurate differential diagnosis with other dermatoses and help confirm the diagnosis in uncertain cases.
5. How long does the procedure take, and how long will results take?
Tissue sampling typically takes no more than 15 to 20 minutes. The specimen is then sent for further evaluation, which may include histopathology, immunohistochemistry, or molecular genetic testing, depending on the clinical indication. Results are usually available within 5 to 14 days, based on complexity and whether additional studies are required.
6. Will a scar remain after a biopsy?
The degree of scarring depends on the biopsy method. After a shave biopsy, sutures are usually not needed, and only a small mark may remain. With punch biopsy or excisional biopsy of skin lesions, sutures are typically placed. As a result, a thin linear scar may remain at the suture site, and it usually fades over time and becomes less noticeable.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Greenwood, J. D., Merry, S. P., & Boswell, C. L. (2022). Skin biopsy techniques. Primary Care. 2022 Mar;49(1):1-22. doi: 10.1016/j.pop.2021.10.001. Epub 2022 Jan 5. PMID: 35125151.
3.
Ramsey, M. L., Conrad, E., Chen, R. L., & Rostami, S. (2025, September 15). Skin biopsy. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan–. PMID: 29262109.
4.
Yasui, Y., Kato, H., Oda, T., Nakamura, M., & Morita, A. (2023). Complications and risk factors of punch biopsy: A retrospective large-scale study. The Journal of Dermatology. 2023 Jan;50(1):98-101.