Post-infarction Rupture of the Papillary Muscle: Etiopathogenesis, Symptoms, Diagnosis, and Treatment
Oleg K.Cardiovascular surgeon, MD
9 min read·January 29, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Post-infarction rupture of the papillary (papilliform) muscle is a rare but extremely life-threatening mechanical complication of acute myocardial infarction, most often leading to acute severe mitral regurgitation (MR), rapid development of pulmonary edema, and/or cardiogenic shock.
This complication most frequently develops within 2–7 days after myocardial infarction, and although the incidence of papillary muscle ruptures is less than 0.5% of all myocardial infarctions, mortality without urgent surgical intervention can exceed 50–80%.
Etiology and pathogenesis
Post-infarction rupture of the papillary muscle results from transmural myocardial infarction, leading to ischemic necrosis of papillary muscles and loss of their mechanical strength. Let us review the key stages of pathogenesis:
Occlusion of the coronary artery
Rupture most frequently occurs due to disruption of blood flow in the territory of the right coronary artery or the circumflex branch. This is generally associated with a single coronary supply to the posteromedial papillary muscle, whereas the anterolateral muscle often has a dual blood supply, which makes it more resistant to ischemia and less likely to lead to rupture.
Thrombotic occlusion of the coronary artery associated with the critical narrowing by the atherosclerotic plaque: 3D model
Ischemic necrosis and mechanical failure of the papillary muscle
Typically, within 2–7 days post-infarction, coagulation necrosis of the myocardium occurs, followed by destruction of the intercellular matrix, leading to a sharp reduction in the mechanical strength of the muscular tissue. At the same time, the weakened muscle undergoing hemodynamic stress (chordal tension) is subjected to partial or complete rupture.
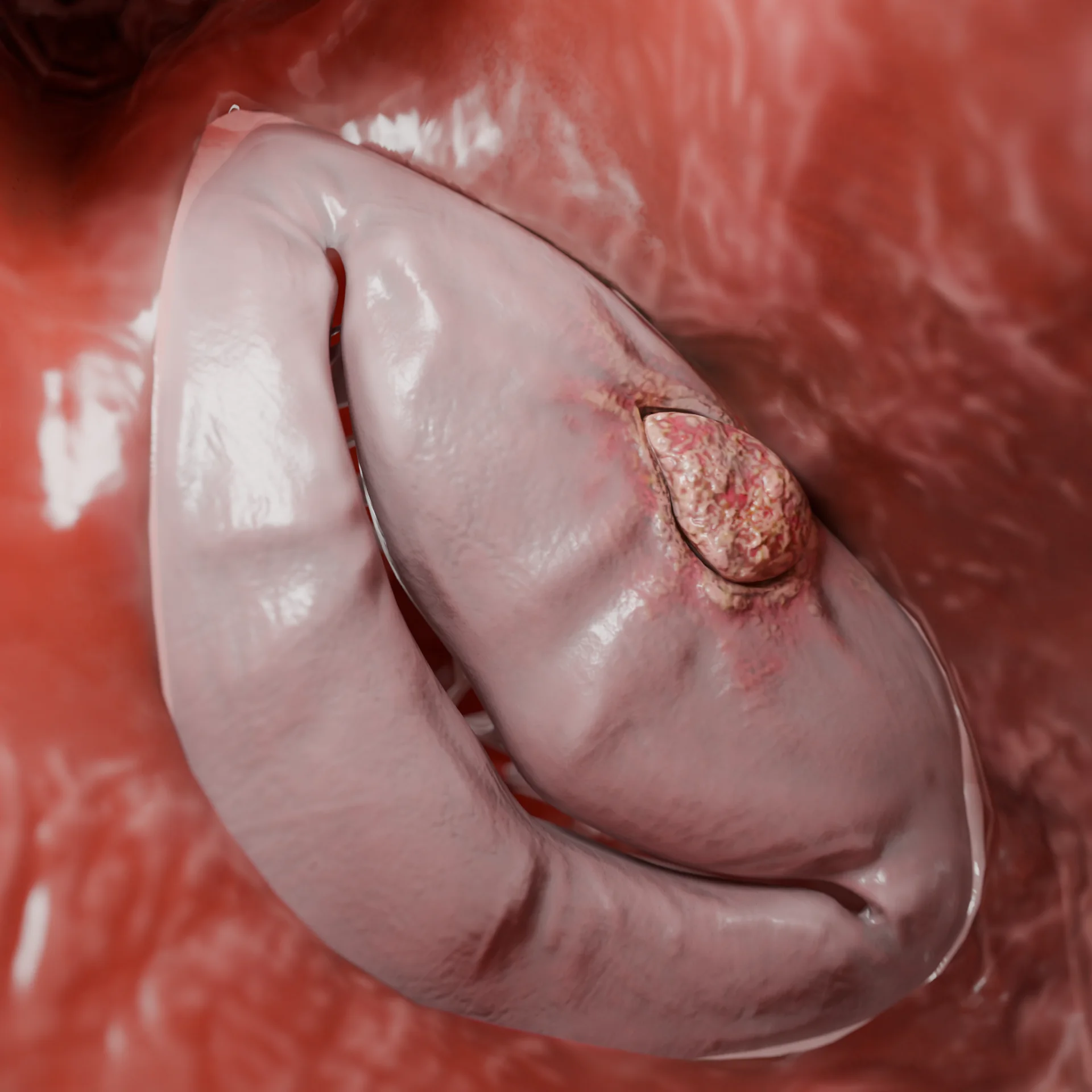
1 – zone of myocardial infarction, 2 – avulsion of papillary muscle: 3D model
Acute mitral regurgitation
The leaflets of the mitral valve cease to coapt because a large segment of the leaflet begins to dislocate into the right atrium in the absence of chordal tension. As a result, a significant portion of blood returns to the left atrium during left ventricular contraction.
Pulmonary edema and cardiogenic shock
A sharp rise in left atrial pressure leads to acute pulmonary edema. Meanwhile, the fall in effective cardiac output leads to cardiogenic shock and organ hypoperfusion. The neurohumoral response to the decrease in cardiac output involves increased vascular resistance, further exacerbating the situation.
Classification of papillary muscle ruptures
By rupture extent
Partial (hemodynamics may be more stable);
Complete.
By involved muscle
Posteromedial;
Anterolateral.
1 – anterolateral papillary muscle, 2 – posteromedial papillary muscle: 3D model
Clinical manifestations
An abrupt clinical deterioration in the patient’s condition is typical for post-infarction rupture of the papillary muscle, generally associated with apparent stabilization after acute myocardial infarction. Onset is mostly reported 2-7 days post-infarction.
Key clinical symptoms include:
Acute dyspnea, rapidly progressing to orthopnea and respiratory failure.
Acute pulmonary edema, often with pink frothy sputum.
Hypotension and tachycardia due to a sharp decrease in effective cardiac output (cardiogenic shock).
A systolic murmur near the heart apex may be faint or absent despite severe mitral regurgitation due to rapid pressure equalization between the left ventricle and atrium.
With partial rupture of the papillary muscle, symptoms may develop less rapidly, which can sometimes result in delayed diagnosis.
Diagnosis of papillary muscle ruptures
We will further discuss the most common diagnostic methods for post-infarction papillary muscle rupture.
Laboratory markers
Laboratory diagnostics do not specifically confirm rupture. Its role is to assess disease severity and complications, as well as to make predictions and select strategies. The main markers of laboratory diagnostics include:
Troponin (hs-cTn). Its elevation confirms acute myocardial injury and allows ischemia to be evaluated dynamically.
BNP/NT-proBNP. The elevation reflects acute pressure/volume overload.
Creatinine, ALT, AST. Markers of organ dysfunction.
Instrumental methods
Echocardiogram
It’s a critical and decisive diagnostic method, which includes:
Transthoracic Echo. First-line method, performed immediately upon clinical suspicion.
Main parameters for evaluation:
Mobility and integrity of the papillary muscles;
Presence of a floating fragment in the left ventricle or left atrium;
Degree of mitral regurgitation (color Doppler); positive signs of pulmonary hypertension;
Dimensions and function of the left ventricle and left atrium;
The width of the vena contracta and density of the continuous Doppler signal are key indicators for identifying significant MR;
Spectral display of MR flow velocity during Doppler often shows a characteristic triangular shape (instead of the typical rounded form for chronic MR).
Transesophageal Echo. It offers significant advantages if the patient’s condition allows for its performance:
High-quality acoustic window;
Allows for more accurate determination of rupture and mitral regurgitation mechanisms, including preoperative planning.
Avulsion of the papillary muscle on echocardiography
Coronary angiography
This method is mandatory for assessing the coronary bed and planning myocardial revascularization.
Examples of angiographies: 1 – subocclusion of the right coronary artery; 2 – critical stenosis of the anterior interventricular branch; 3 – occlusion of the circumflex branch
Right heart (pulmonary artery) catheterization
The method allows for the recording of large V-waves during pulmonary artery wedge pressure (PAWP) measurement, which is a typical sign for acute severe mitral regurgitation.
Treatment
Medical therapy
In this case, medical therapy serves as a temporary measure to stabilize breathing and hemodynamics. It is considered as part of preparation for urgent surgical treatment or, for certain patients, for percutaneous intervention/mechanical circulatory support. Medical treatment options include:
Respiratory support. Non-invasive ventilation (NIV) with continuous positive airway pressure (CPAP). In cases of severe respiratory failure, use mechanical ventilation with positive end-expiratory pressure (PEEP).
Diuretics (more often, the loop diuretics: furosemide/torasemide). Used to off-load the pulmonary circulation.
Vasodilators (sodium nitroprusside or nitrates). Contraindicated in hypotension.
Inotropes (dobutamine, milrinone). Recommended for low output and signs of hypoperfusion.
Vasopressors (norepinephrine). Used in severe hypotension. Often used together with inotropes.
Surgical therapy
Emergency surgery. Prioritized for patients with acute mitral regurgitation due to papillary muscle rupture. In the case of a full rupture, mitral valve replacement is more frequently performed.
Valve repair. Most often performed in cases of partial rupture, relative patient stability, and high team expertise.
Coronary artery bypass grafting. Often performed in cases of significant coronary artery lesions. This type of surgery is performed under cardiopulmonary bypass through median sternotomy.
Minimally invasive approaches are allowed in situations of relative stability, individually, when there is no need for coronary artery bypass grafting and with high team expertise.
Mechanical circulatory support
For patients with acute mitral regurgitation and cardiogenic shock, temporary stabilization can be achieved using short-term circulatory support devices. These include:
Intra-aortic balloon pump (IABP), or counterpulsation;
Percutaneous transaortic left ventricle support device (e.g., Impella);
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Endovascular treatment
Transcatheter edge-to-edge repair (TEER, e.g., MitraClip) can be considered for patients at extremely high surgical risk, often as a bridge to open surgery in particular cases and with suitable anatomy. Currently, there is still not an extensive evidence base for this method.
FAQ
1. What is post-infarction papillary muscle rupture?
It is a rare mechanical complication of myocardial infarction, leading to acute severe mitral regurgitation and life-threatening hemodynamic instability.
2. How often does papillary muscle rupture occur?
In the era of modern reperfusion therapy, it occurs in less than 0.5% of patients with myocardial infarction.
3. When does papillary muscle rupture most often develop?
Usually on the 2nd to 7th day after myocardial infarction.
4. Which papillary muscle is more commonly affected, and why?
The posteromedial papillary muscle, usually due to a single coronary blood supply.
5. What are the main symptoms indicating papillary muscle rupture?
6. Which diagnostic method is key in identifying papillary muscle rupture?
Echocardiography: transthoracic echocardiography (TTE) with subsequent transesophageal echocardiography (TEE), if necessary.
7. Can papillary muscle rupture be treated with medical therapy alone?
No, medical therapy is only used temporarily for stabilization before surgical intervention.
8. What is the standard treatment method for papillary muscle rupture?
Urgent surgical intervention, most often mitral valve replacement.
9. Are there any alternative treatment methods for papillary muscle rupture besides surgery?
In certain cases, for patients at high surgical risk, transcatheter methods (TEER) may be used as a bridge or an alternative to surgery.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: VOKA Catalog. https://catalog.voka.io/
2.
Fujita, T., Yamamoto, H., Kobayashi, J., et al. (2020, December). Mitral valve surgery for ischemic papillary muscle rupture: Outcomes from the Japan Cardiovascular Surgery Database. General Thoracic and Cardiovascular Surgery, 68(12), 1439–1446. DOI: 10.1007/s11748-020-01418-y.
3.
Yousef, S., Sultan, I. (2022, January). Surgical repair for post-infarction papillary muscle rupture: Where do we stand? European Journal of Cardio-Thoracic Surgery, 61(2), 477–478. DOI: 10.1093/ejcts/ezab534.
4.
Kaczorowski, D. J., Takeda, K., Atluri, P., et al. (2025, November). 2025 American Association for Thoracic Surgery (AATS) Expert Consensus Document: Surgical management of acute myocardial infarction and associated complications. Journal of Thoracic and Cardiovascular Surgery, 170(5), 1327–1344. DOI: 10.1016/j.jtcvs.2025.04.013.
5.
Massimi, G., Ronco, D., De Bonis, M., et al. (2022, January). Surgical treatment for post-infarction papillary muscle rupture: A multicentre study. European Journal of Cardio-Thoracic Surgery, 61(2), 469–476. DOI: 10.1093/ejcts/ezab469.
6.
Chang, C. W., Romero, S., & Price, M. J. (2022, August). Transcatheter edge-to-edge repair for acute mitral regurgitation due to postinfarction papillary muscle rupture. Journal of the Society for Cardiovascular Angiography & Interventions, 1(5), 100431. DOI: 10.1016/j.jscai.2022.100431.
7.
Russo, A., Suri, R. M., Grigioni, F., et al. (2008, October). Clinical outcome after surgical correction of mitral regurgitation due to papillary muscle rupture. Circulation, 118(15), 1528–1534. DOI: 10.1161/CIRCULATIONAHA.107.747949.
8.
Moursi, M. H., Bhatnagar, S. K., Vilacosta, I., et al. (1996, September). Transesophageal echocardiographic assessment of papillary muscle rupture. Circulation, 94(5), 1003–1009. DOI: 10.1161/01.cir.94.5.1003.