Invasive Hemodynamic Monitoring in Anesthesiology: Types, Indications, and Possible Complications
Irina K.ICU doctor, MD
11 min read·February 12, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Invasive hemodynamic monitoring is a method of controlling the physiological parameters of the body, requiring catheterization of vessels and/or the introduction of sensors into the heart cavities or large vessels for continuous and more reliable measurement of hemodynamic parameters and rapid receipt of laboratory data.
These monitoring methods have several objectives: determining hemodynamic status to ensure optimal perfusion and functioning of target organs, monitoring the volume of circulating blood and the body’s response to intensive measures taken, as well as potentially earlier detection of cardiovascular dysfunction.
Main types of invasive monitoring used in a surgery room:
Invasive blood pressure monitoring;
Central venous catheterization;
Pulmonary artery catheterization (PAC).
Indications for use
Effective invasive hemodynamic monitoring combined with competent clinical decision-making can improve patient treatment outcomes. However, the application of invasive monitoring methods is justified when the benefit of obtaining clinical data and adjusting patient management tactics outweighs the potential risks of use.
Understanding the operating principles of each monitoring device, indications for its use, risks, and limitations is crucial when choosing a monitoring method.
Indications for use can be divided into three groups:
Intervention characteristics (cardiothoracic, vascular, thoracic, neurosurgical, large abdominal, and trauma surgeries with a high risk of blood loss);
Assessment of patient condition (severe cardiovascular disorders, multiple organ failure, septic shock, and any other conditions that may lead to hemodynamic disturbances);
Need for intensive control and therapy (use of inotropic and vasopressor drugs, need for frequent blood tests).
Invasive blood pressure monitoring
Invasive blood pressure monitoring is a method of continuously measuring blood pressure using an arterial catheter connected to a fluid-filled system and a pressure sensor (transducer). The sensor forms a blood pressure waveform and also allows for frequent sampling of arterial blood for analysis of blood gases, acid-base balance (ABB), electrolytes, hemostasis, and other laboratory indicators.
With proper use, direct intra-arterial monitoring is more accurate than non-invasive blood pressure measurement.
Indications for intra-arterial catheterization
Anticipated hemodynamic instability, as well as the need for vasopressor support;
High risk of organ dysfunction in hypotension (elderly patients, patients with coronary artery disease [CAD] or chronic kidney disease [CKD]);
Inability to accurately measure blood pressure with a cuff (patients with obesity, tremors, or arrhythmias).
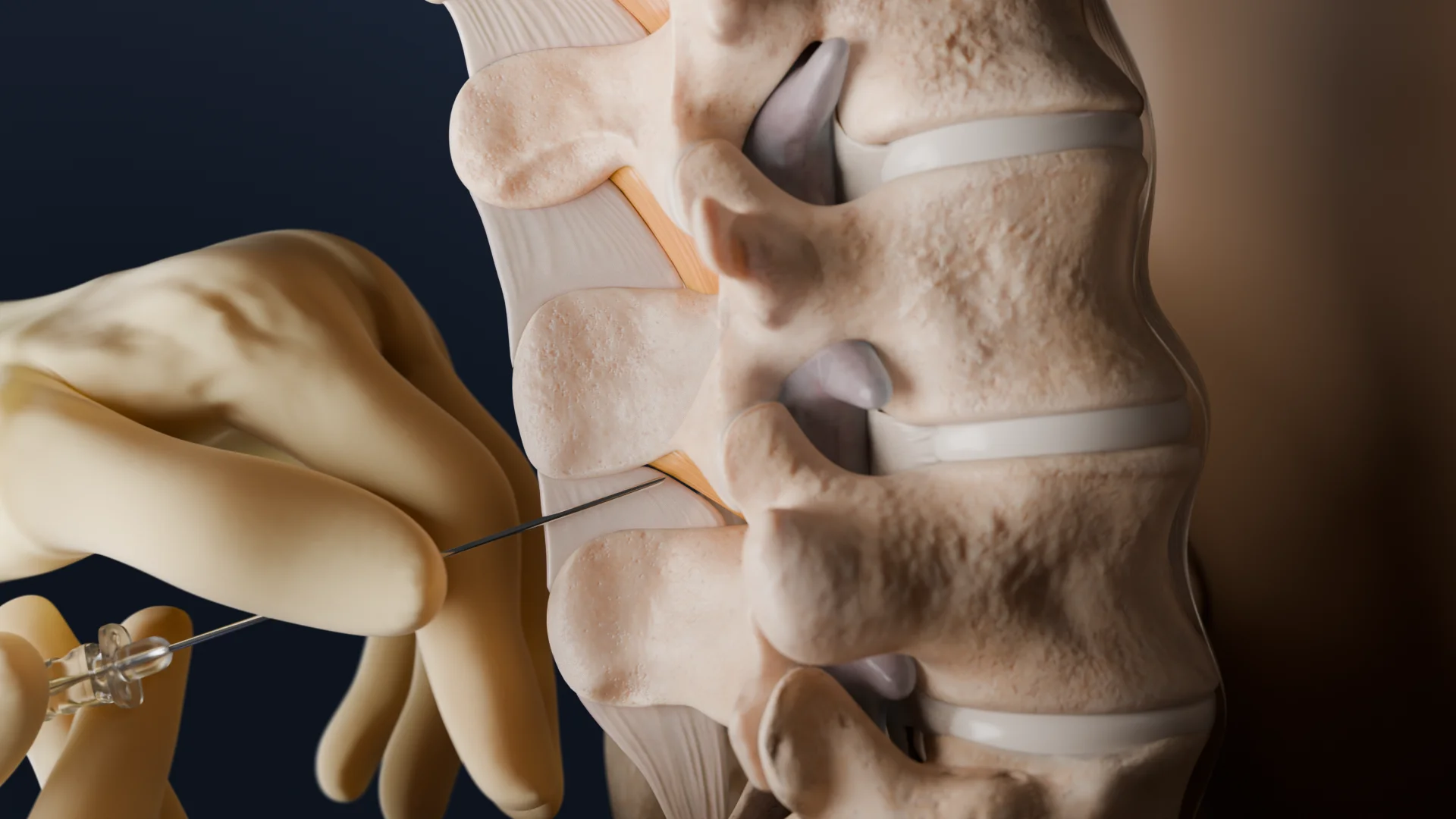
Technical aspects of catheterization and monitoring
In patients with indications for monitoring, the arterial catheter should be placed before anesthesia induction.
Arterial catheters should primarily be inserted into the radial artery (this location is preferred due to the presence of collateral circulation in the hand, easy accessibility, and compressibility, providing less risk of serious complications).
Alternative commonly used sites for arterial monitoring include the following:
Femoral artery;
Brachial artery;
Axillary artery;
Dorsalis pedis artery.
In some clinical cases, femoral access is preferred (peripheral vasospasm in cardiogenic shock, Buerger’s disease, and in some cases during the surgery for dissecting aortic aneurysm, where it is preferable to use two arterial accesses).
Arterial catheters of smaller diameter (20G) are associated with a lower risk of complications. The use of ultrasound navigation is preferable during catheterization.
The pressure sensor requires correct alignment (“right atrium level”) and zeroing relative to atmospheric pressure (each time the patient is repositioned, the zeroing maneuver should be performed).
In all positions where the “right atrium level” is below the base of the skull, the pressure sensor should be set at the level of the base of the skull.
Mean arterial pressure should be maintained at a level above 65 mm Hg.
Optimal quality of the blood pressure waveform is essential for accurate measurement and interpretation of the obtained data. Two types of artifacts can alter signal quality: insufficient damping (resonance) and excessive. In the first case, the causes are a faulty pressure sensor or an excessively stiff arterial line. Excessive resonance occurs when there are bubbles, blood clots in the circuit, open connections, kinks, or catheter obstructions.
3D animation: radial artery catheterization using the Seldinger technique
Complications
The most common complications of intra-arterial catheterization are as follows:
Local pain and paresthesia;
Hematoma and minor bleeding at the puncture site.
Less common complications include the following:
Severe bleeding;
Air or thrombotic embolism;
Arterial thrombosis;
Formation of pseudoaneurysm;
Local nerve damage.
Central venous catheterization
This is an invasive medical procedure widely used in patients for measuring central venous pressure (requires cautious interpretation) and parameters of venous oxygenation, as well as providing reliable access for continuous drug administration (safe administration of inotropes and vasopressors, hyperosmolar solutions, and prolonged infusions).
Indications for central venous catheterization
Need for vasoactive support during surgery and in the postoperative period;
High risk of intraoperative massive blood loss and the need for rapid venous access;
Need for monitoring of central venous pressure (CVP).
Technical aspects of central venous catheterization
Target veins for central venous catheterization include central veins of the chest (e.g., subclavian vein, internal jugular vein) or veins of the iliac-caval venous system (e.g., common femoral vein). Catheterization is performed using the Seldinger technique.
Upper extremity accesses are preferred due to a lower thrombotic risk compared to femoral access. The choice of puncture site should be determined based on clinical necessity. Areas with higher risks (skin with signs of infection or burns) should be avoided. Patient positioning (e.g., Trendelenburg position) for upper access, if clinically permissible.
Central venous catheterization should be performed in a place where sterile manipulations can be carried out, and the presence of an assistant during catheterization is necessary. Ultrasound navigation is recommended during venous puncture and as a method of confirming the correct position of the guidewire. Basic monitoring should also be ensured during the manipulation so that any complications are quickly detected and managed.
The use of a closed infusion system reduces the risk of mortality and sepsis caused by catheter-associated bloodstream infections.
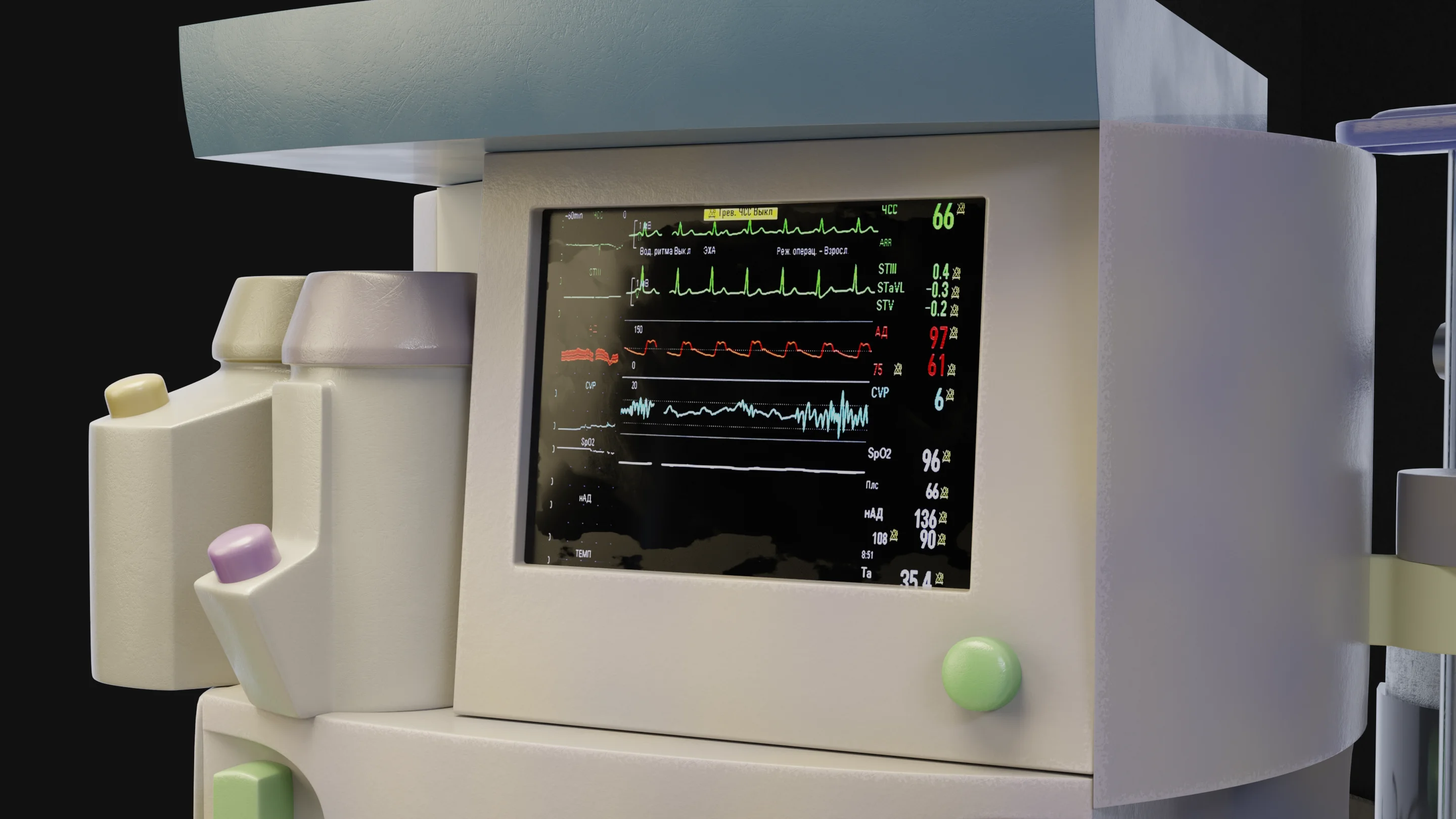
Continuous monitoring of CVP is performed with a venous catheter connected to a fluid-filled system (without kinks, blood clots, and air) and a pressure sensor (transducer) forming a CVP waveform representing pressure changes in the right atrium. For a correct waveform, the catheter tip should be positioned without touching the vein wall, the sensor zeroed relative to atmospheric pressure, and positioned at the level of the right atrium.
CVP should be considered one of the trends in assessing volume status (along with blood pressure, echocardiography (point-of-care ultrasound [POCUS]: e.g., inferior vena cava variability), clinical perfusion, and diuresis).
Complications of central venous catheterization
Erroneous puncture of a nearby artery (carotid artery, subclavian, or femoral) with hematoma formation: local hemostasis can be achieved by compression, occasionally requiring a vascular surgeon;
Pneumothorax is manifested by symptoms such as cough, difficulty breathing, and chest pain, as well as x-ray or ultrasound data (requires air drainage if it occupies at least 30% of the thoracic cavity and is accompanied by clinical symptoms);
Hemothorax, hemomediastinum, and cardiac tamponade: caution should be exercised in patients who have undergone multiple punctures during catheterization;
Local nerve damage during puncture or nerve compression by a resulting hematoma;
Pleural effusion: extravasation of infused fluid in case of vessel damage;
Air embolism: accidental entry of air through the puncture needle during catheterization, requiring Valsalva maneuver or tilting the head downwards;
Arrhythmia: mechanical stimulation by the guidewire can cause supraventricular tachycardia or ventricular fibrillation;
Damage to the thoracic duct with the development of chylothorax.
The pulmonary artery catheter is a multi-lumen catheter introduced through a central vein (predominantly via the right internal jugular vein), guided through the right side of the heart into the pulmonary artery for hemodynamic monitoring. This allows monitoring of hemodynamic variables related to the function of both the right and left sides of the heart, such as:
Continuous cardiac output (CO) measurement;
Pulmonary artery pressure (PAP);
Pulmonary artery wedge pressure (PAWP);
Right ventricular ejection fraction (RVEF);
Right ventricular end-diastolic volume (RVEDV);
Tissue perfusion variables (oxygenation of mixed venous blood).
This method should not be used routinely when less invasive technology (echocardiography) can provide the necessary information to the physician.
Catheter components
The body of the catheter with centimeter markings for depth determination;
The distal lumen opens at the tip of the catheter, located in the pulmonary artery (PAP measurement);
The proximal lumen opens at the tip of the catheter, located in the right atrium (CVP measurement);
Balloon located at the distal end (when temporarily inflated [1.5 ml of air] performs PAWP measurement);
Thermistor at the distal end (CO measurement via thermodilution);
Additional lumens depending on various models (port for constant thermodilution, optical module for mixed venous saturation measurement);
Proximal connectors with various color coding for connection to pressure sensors and monitoring systems.
Swan-Ganz catheter
Indications for pulmonary artery catheterization
Heart transplantation;
Severe hemodynamic instability accompanied by shock of any type for escalation and de-escalation of therapy;
Diagnosis of pulmonary hypertension;
Complex cardiac surgeries;
Evaluation and management of patients after heart and lung transplantation and in the assessment of porto-pulmonary hypertension in patients requiring liver transplantation;
Hemodynamic monitoring during initiation and weaning from veno-arterial extracorporeal membrane oxygenation.
Contraindications
The absolute and relative contraindications for catheterization of the right side of the heart include the following:
Severe coagulopathy;
Presence of a newly implanted endocardial pacemaker (PM);
Septal defect following myocardial infarction;
Right-sided endocarditis;
Risks of atrial or ventricular perforation.
Complications of PA catheterization
Complications arising from puncture (corresponding to central venous catheterization complications);
Complications during catheter insertion (valve damage, myocardial perforation, air embolism upon balloon rupture);
Complications occurred when the catheter was inserted (thromboembolism of the right segments, pulmonary valve endocarditis, and pulmonary artery rupture).
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Conclusion
Invasive hemodynamic monitoring holds an important place in anesthesiology and perioperative intensive care as a tool for continuous high-sensitivity assessment of circulation in patients at high risk for complications, helping physicians expedite the recognition of hemodynamic instability, and provide targeted correction of volume status, vascular tone, and inotropic support.
FAQ
1. What is included in invasive hemodynamic monitoring?
Arterial line, central venous catheter (CVC) with CVP/ScvO₂ measurement (as indicated), and cardiac output monitoring methods via pulmonary artery catheter placement in specific situations.
2. When is invasive arterial pressure monitoring (arterial line) mandatory?
When rapid BP fluctuations are expected, continuous control and/or frequent arterial blood analyses are needed, vasoactive therapy is indicated, or significant blood loss is anticipated.
3. Why perform central venous catheterization with available peripheral access?
For reliable administration of vasopressors/concentrated infusions, complex access, massive infusion-transfusion therapy, and prolonged intensive management.
4. Can CVP evaluate “blood volume” and infusion needs?
No. CVP poorly predicts infusion response; it is mainly used as a trend in the context of clinic, ventilation, and RV function.
5. When are cardiac output monitoring methods needed?
In high-risk patients and/or during high-risk surgeries, when it is important to understand the reason for hypotension and assess the effects of fluids, vasopressors, and inotropes.
6. In which cases is PAC preferred?
In complex cardiopulmonary pathology and refractory instability (cardiogenic/mixed shock, severe pulmonary hypertension, severe right ventricular failure) when less invasive methods do not provide answers and PAC data alters management.
7. What are the most significant complications of invasive monitoring in practice?
For arterial catheter: ischemia/thrombosis, hematoma, infection; for CVC: arterial puncture, pneumothorax, misalignment, air embolism, infection/thrombosis; for pulmonary artery catheterization: arrhythmias, perforation of the PA (rare but severe).
8. What is the main practical principle of using invasive monitoring?
Deploy when it genuinely impacts decisions, and interpret the data critically and comprehensively in conjunction with clinical, laboratory, and POCUS/echo results.
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Vojnar B., Achenbach P., Flick M. (2025). Haemodynamic monitoring and management during non-cardiac surgery: a survey among German anaesthesiologists. Journal of Clinical Monitoring and Computing. 39(5):853–861. doi: 10.1007/s10877-025-01284-0
3.
Saugel B., Kouz K., Meidert A.S. (202). How to measure blood pressure using an arterial catheter: a systematic 5-step approach. Critical Care. 24:172. doi: 10.1186/s13054-020-02859-w.
4.
Gilbert-Kawai N., Chen R., Patel S. (2024). Pulmonary artery catheterisation. British Journal of Anaesthesia. 24(12):447-457. DOI: 10.1016/j.bjae.2024.08.003