Basic Monitoring During Anesthesia: Standards and Mandatory Monitoring Parameters
Analysis of basic monitoring standards during anesthesia. Mandatory parameters of oxygenation, ventilation, and hemodynamics for patient safety.
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders
Anesthesia
Pain management and sedation techniques
Angiology
Arterial and venous pathologies
Cardiology
Acquired and congenital heart diseases
Dentistry
Diseases of teeth, gums, and the oral cavity
Dermatology
Disorders of the skin and subcutaneous tissue
Endocrinology
Disorders of the glands and hormonal imbalance
Gastroenterology
Stomach, intestinal, and digestive diseases
Gynecology
Diseases of female reproductive organs
Hepatology
Liver, gallbladder, and biliary tract diseases
Neurology
Brain, spinal cord, and peripheral nerve disorders
Obstetrics
Pregnancy complications and abnormal fetal positions
Oncology
Cancer types, benign and malignant tumors
Ophthalmology
Conditions affecting the eyes and vision
Otorhinolaryngology
Ear, nose, and throat diseases
Pediatrics
Child health, development, and clinical conditions
Physiology
Biological processes within organs and systems
Pulmonology
Lung and respiratory tract diseases
Traumatology
Acute injuries and musculoskeletal trauma
Urology
Urinary tract and male reproductive disorders

This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
General anesthesia (GA) is a controlled, reversible state characterized by loss of consciousness, amnesia, analgesia, muscle relaxation or immobility, and attenuation of adverse autonomic responses to painful stimuli. This state serves to maintain physiological homeostasis during surgical and other interventional procedures.

Before administering anesthesia, all patients undergo an assessment of their health status, potential perioperative risks, and readiness for the planned procedure.
Evaluating perioperative risks helps identify vulnerable patients in advance, optimize comorbidities, determine the anesthesia plan (required monitoring, infusion strategy, postoperative observation), and conduct patient counseling, including discussion of expected risks and obtaining informed consent.
In clinical practice, the ASA Physical Status Classification is widely used as a basic indicator of patient severity, along with other scales such as the ACS NSQIP Surgical Risk Calculator for non‑cardiac surgical patients and the RCRI for assessing cardiovascular complications.
Modern GA includes three stages:
Induction is the process of bringing the patient into an unconscious state by administering an adequate concentration of anesthetic, followed by continued maintenance of anesthesia. Induction is the most vulnerable stage, during which the patient transitions within minutes from preserved protective reflexes to apnea and potential hypotension.
Safety is ensured through prior preparation:
Induction may be achieved intravenously or via inhalation, depending on the clinical situation or patient age. Among adults, intravenous induction is preferred and typically includes a hypnotic agent (propofol, etomidate, ketamine), an adjuvant (an opioid and/or benzodiazepine), and a neuromuscular blocking drug if intubation is planned.
Inhalational anesthesia is often added as a supplemental component after initial loss of consciousness with IV hypnotics, or used as the sole method.
Airway management is an integral part of GA, ensuring adequate ventilation and oxygenation, as well as delivery of the anesthetic gas mixture.
Airway Accessories
Special situations: Include high aspiration risk (requiring rapid sequence induction, RSI) and difficult airways.
The primary goal of this stage is to maintain Stage 3 surgical anesthesia at a safe depth, particularly in elderly patients and those with significant comorbidities. This includes:
Maintenance may rely primarily on inhalational or intravenous techniques. An ideal anesthetic should exhibit:
No currently available anesthetic is ideal for all patients; all anesthetic agents have potential side effects.
Thus, maintenance may involve inhalational anesthetics alone, total intravenous anesthesia (TIVA), or one or more inhalational agents in combination with several intravenous sedatives and analgesics (opioid and nonopioid), with or without additional neuromuscular blockers.
These agents produce loss of consciousness and may also provide additional effects, including analgesia (nitrous oxide) and muscle relaxation (isoflurane). All inhalational anesthetics are either pressurized liquefied gases or volatile liquids. Potency is measured by the minimum alveolar concentration (MAC), defined as the concentration that prevents movement in response to a surgical stimulus in 50 % of patients at 1 atm.
Inhalational anesthetics include:
Advantages of inhalational anesthesia:
Disadvantages:
These agents produce rapid loss of consciousness when administered in appropriate doses (typically achieved after one arm‑brain circulation time). Maintenance of GA exclusively through intravenous (IV) administration is called total intravenous anesthesia (TIVA).
Infusion doses are adjusted based on age, BMI, frailty, and comorbidities. Synergism is achieved when combining IV anesthetics from different classes, allowing dose reduction of each agent.
Key components of IV anesthesia:
Advantages of TIVA:
Disadvantages of TIVA:
Muscle relaxants, or neuromuscular blocking drugs (NMBDs), are divided into two classes based on their mechanism of action:
Selection of a specific NMBD is based on the planned duration of the surgical procedure and the presence of severe renal or hepatic dysfunction.
Advantages of NMBDs:
Disadvantages and Risks of NMBDs:
This stage signifies a gradual return of consciousness after anesthetics and adjuvant medications are discontinued at the end of the procedure, allowing the patient to transition smoothly from surgical anesthesia to wakefulness.
Key objectives of this stage:
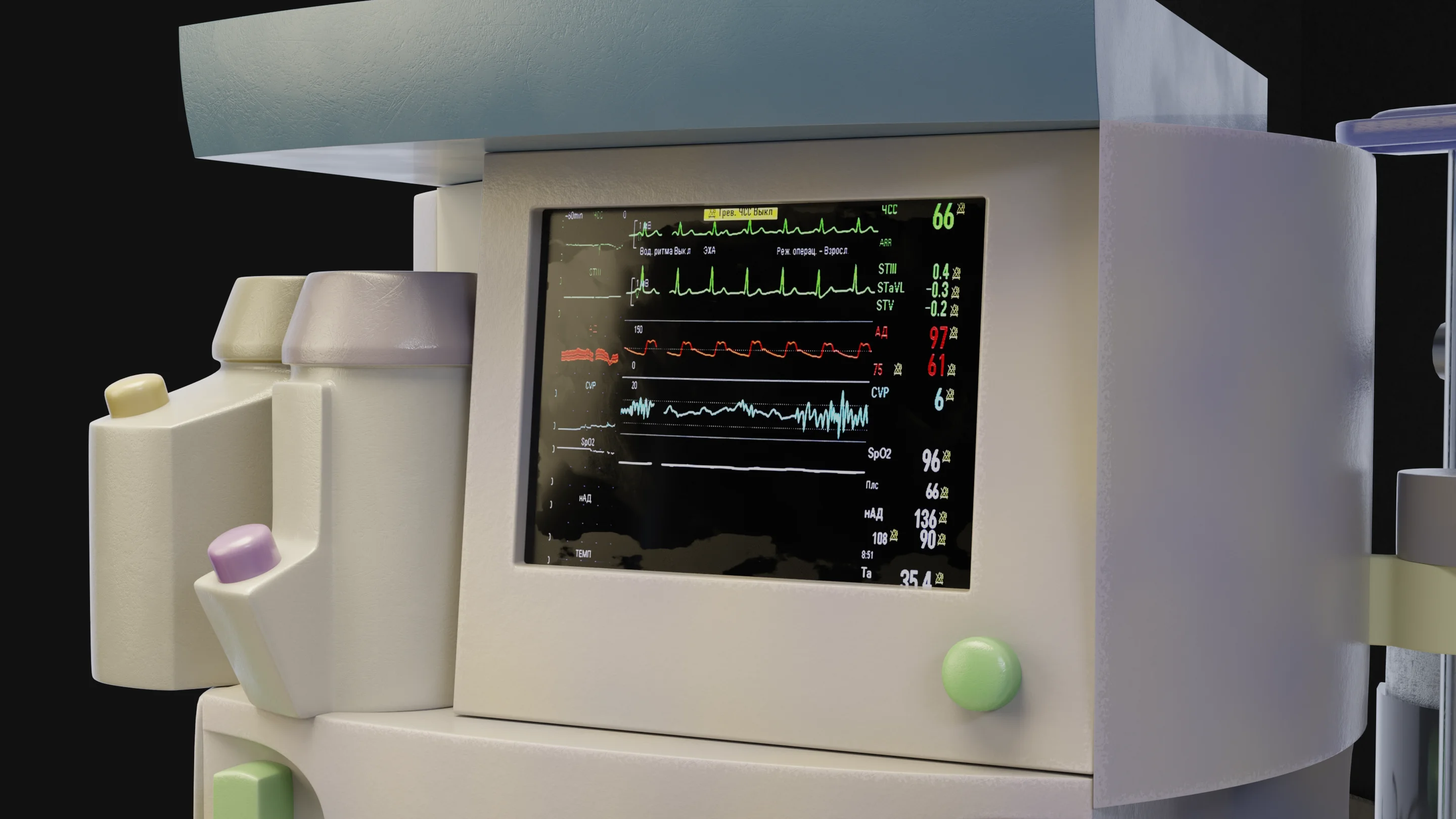
Monitoring is a fundamental and mandatory component of GA. The anesthesiologist must continuously assess the patient’s physiological variables as well as anesthesia equipment parameters, since anesthesia and surgery can cause rapid changes in vital signs.
Find more scientifically accurate content on our social media








Most patients are transported to the PACU after anesthesia to ensure timely management of postoperative side effects. Critically ill patients — whether conscious or intubated — are transported to the ICU for further treatment.
1. What is general anesthesia and how does it affect the body?
2. What is the difference between local and general anesthesia?
3. How dangerous is general anesthesia in modern medicine?
4. Are “general anesthesia” and “narcosis” the same thing?
5. What medications are used for anesthesia?
6. What effects may patients experience after emergence?
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Nimmo, A.F., Absalom, A.R., Bagshaw, O. (2019). Guidelines for the safe practice of total intravenous anaesthesia (TIVA): Joint Guidelines from the Association of Anaesthetists and the Society for Intravenous Anaesthesia. 74(2):211-224. doi: 10.1111/anae.14428.
3.
Khorsand, S.M. Maintenance of general anesthesia [Internet]. In: Post TW, editor. UpToDate [Internet]. Waltham (MA): UpToDate; 2025 [updated 2025 Mar 5; cited 2025 Dec].
4.
Saugel, B., Buhre, W., Chew, M.S. (2025). Intra-operative haemodynamic monitoring and management of adults having noncardiac surgery. European Journal of Anaesthesiology 42(6):p 543-556, DOI: 10.1097/EJA.0000000000002174.
5.
Ludovico, F., Pietro, Di F., Patrick, Del M. (2024). Anesthetic gases environmental impact, anesthesiologists’ awareness, and improvement opportunities: a monocentric observational study. Journal of Anesthesia, Analgesia and Critical Care 4:47. doi: 10.1186/s44158-024-00183-1.
Loading test 6 questions




Summarize article with AI
Choose your preferable AI assistant:
Link successfully copied to clipboard
Thank you!
Your message is sent!
Our experts will contact you shortly. If you have any additional questions, please contact us at info@voka.io