Basic Monitoring During Anesthesia: Standards and Mandatory Monitoring Parameters
Irina K.ICU doctor, MD
7 min read·February 26, 2026
This article is for informational purposes only
The content on this website, including text, graphics, and other materials, is provided for informational purposes only. It is not intended as advice or guidance. Regarding your specific medical condition or treatment, please consult your healthcare provider.
Basic monitoring is a continuous assessment of key physiological parameters of the patient’s body, enabling timely detection of deterioration in oxygenation, ventilation disorders, hemodynamics, thermoregulation, and other potentially life-threatening complications during anesthesia.
International guidelines emphasize that patient safety in the operating room is not only ensured by monitoring but also by the constant presence and clinical evaluation of the anesthesiologist during anesthesia, procedural sedation, and patient transportation, as well as properly adjusted monitoring device alarms.
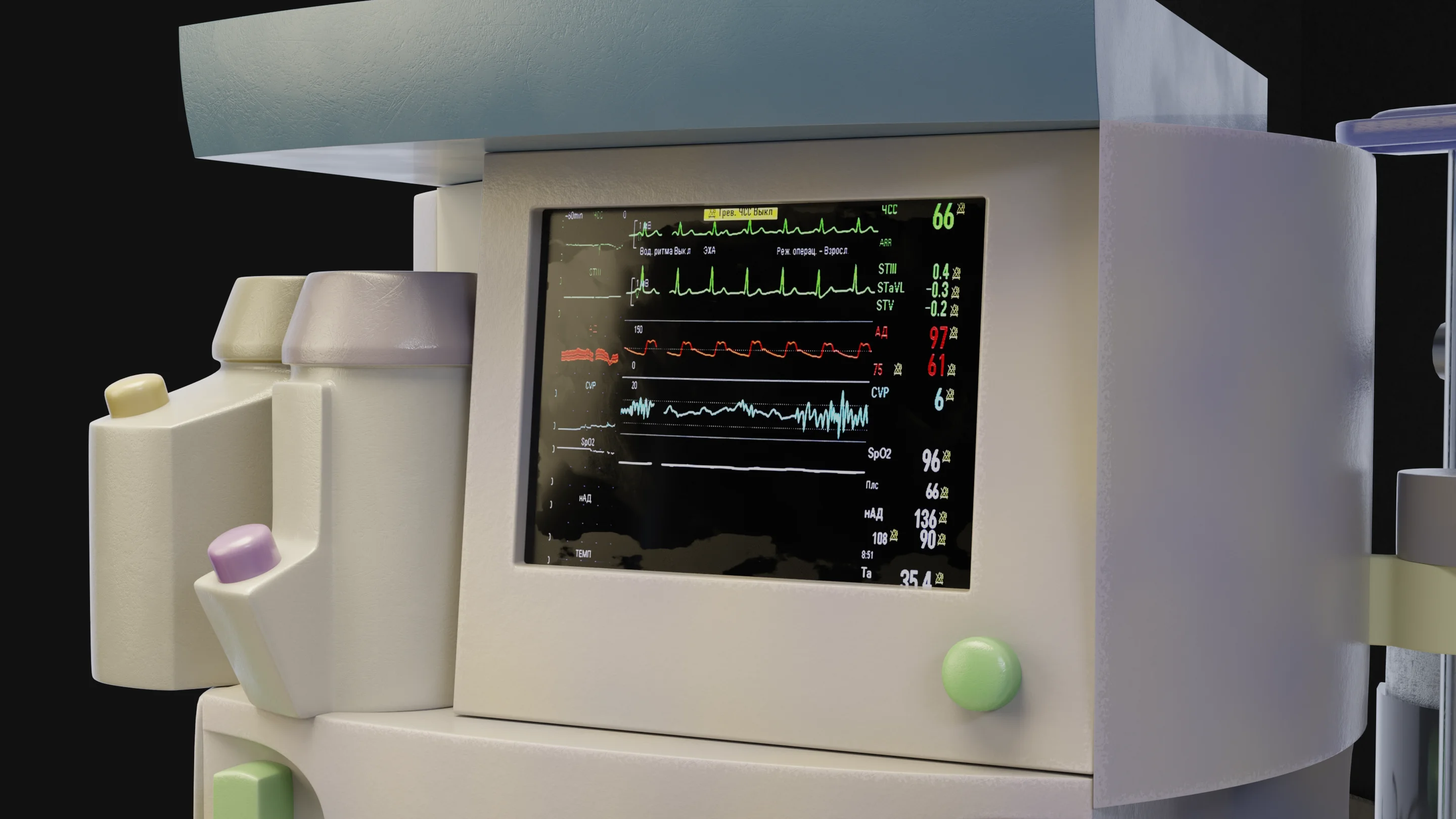
Patient monitor with basic and advanced vital parameters
Control of anesthesiology equipment
The anesthesiologist must check all equipment before use. The anesthesiologist should be properly trained to use all equipment and carry out all specialized equipment checks as recommended by the manufacturers.
The provision, maintenance, calibration, and upgrading of equipment are the responsibility of the institution where anesthesia is performed.
When administering any component of anesthesia via an infusion pump, the device must be checked before use. Infusion pumps must have audible alarms enabled by default.
Monitoring devices
Monitoring of a patient under any type of anesthesia should include regular assessment and recording of parameters for oxygenation, ventilation, and circulation.
The specific scope of monitoring is determined by the clinical situation and type of anesthesia. Thus, the minimum monitoring during anesthesia should include several components.
In all cases:
Pulse oximeter with plethysmography;
Noninvasive blood pressure measurement;
Electrocardiography (ECG);
Temperature measurement before anesthesia and every 30 minutes until the end of the surgery.
During general anesthesia:
Oxygen concentration in inhaled and exhaled air;
Capnography with waveform display.
Depending on the methodology used, the following must be implemented:
Concentration of inhaled anesthetic and nitrous oxide in inhaled and exhaled air when used;
Airway pressure, tidal volume, and respiratory rate during mechanical ventilation;
Quantitative neuromuscular monitoring when muscle relaxants are used, with Train-of-Four (TOF) monitoring target value ≥ 0.9 before extubation;
Processed electroencephalography (pEEG) or bispectral index (BIS) monitoring for total intravenous anesthesia;
Monitoring of blood glucose levels in capillary blood (must be immediately available).
The main physiological parameters requiring monitoring during anesthesia—oxygenation, ventilation, circulation, and thermoregulation—will be discussed in more detail.
Patient monitoring
During anesthesia, the physiological state of the patient and the adequacy of anesthesia must be continuously assessed. For this purpose, monitoring devices are used to complement clinical observation.
Clinical observation includes:
Evaluation of mucous membrane color;
Pupil size, lacrimation, photoreaction;
Chest and/or breathing bag movement;
Absence of reaction to surgical stimuli;
Pulse palpation; auscultation of breath sounds;
Measurement of urine output and blood loss.
Oxygenation monitoring
Oxygenation assessment is performed through clinical assessment of patient skin color (though this method is not always reliable due to factors such as natural skin pigment, room lighting, and hemoglobin concentration), continuous pulse oximetry (SpO₂), and determining oxygen content in the inspired mixture.
Pulse oximetry is a quantitative method of assessing oxygenation. In the operating room, pulse oximeters are usually placed on a finger or earlobe in adults and on the foot/ankle or wrist/palm in infants, allowing light to pass through the tissues and be registered on the other side.
If pulse oximetry cannot be used during anesthesia induction (e.g., in small children or non-cooperative adults), the monitor should be connected immediately after loss of consciousness. Variable pulse tone and low-threshold alarm signals should be audible to the anesthesiologist.
During every general anesthesia with the use of an anesthesia machine, it is mandatory to use an oxygen analyzer, thus preventing the delivery of a hypoxic gas mixture. Contemporary gas analyzers for anesthesia simultaneously measure the concentration of oxygen (O₂), carbon dioxide (CO₂), and inhaled anesthetic.
Ventilation monitoring
During anesthesia, the adequacy of lung ventilation needs to be assessed for all patients. This is achieved through the following clinical observation methods:
Monitoring the chest movements;
Auscultation;
Monitoring the signs of airway obstruction in patients with spontaneous breathing.
It is also necessary to promptly recognize abnormal respiratory sounds that may arise due to improper placement of supraglottic devices, stridor, airway blockage, laryngospasm, or bronchospasm.
Capnography (EtCO₂) is a vital method for monitoring airway patency and alveolar ventilation. Waveform capnography is the gold standard for monitoring intubated airways, as it reliably confirms correct tracheal intubation and diagnoses bronchospasm, hypoventilation, and malignant hyperthermia.
Measurement of lung mechanics is performed by anesthesia-respiratory machines, allowing:
Continuous monitoring of tidal volume, respiratory rate, and minute ventilation;
Control through monitoring of peak, mean, and end-expiratory pressures in the airways in digital and waveform form.
Monitoring of the circulatory system
The adequacy of circulatory function is assessed both through clinical observation and with monitors. Clinical observation is carried out by assessing skin color and temperature, the quality of palpable pulses, and auscultation of heart sounds; urine output can be used to assess organ perfusion.
A standard device for intraoperative non-invasive BP monitoring is an automatic oscillometric cuff, with BP measurements conducted periodically, usually no less frequently than every 5 minutes.
ECG must be continuously monitored during anesthesia. It is a reliable method for monitoring heart rate, rhythm, conduction, and electrolyte disturbances. Standard twelve-lead ECG is not feasible in the operating room. Instead, three or five leads are used.
Temperature monitoring
The majority of patients undergoing general anesthesia, lasting more than 30 minutes, or major surgeries with neuroaxial anesthesia require temperature monitoring.
The patient’s temperature should be monitored for detecting changes (more often hypothermia), managing thermoregulation, and early detection of malignant hyperthermia.
Find more scientifically accurate content on our social media
Subscribe and don’t miss out the latest resources
Documentation of anesthesia
Accurate recording of data from all monitoring devices is necessary. Currently, automated electronic systems for maintaining anesthesia documentation integrated into the patient’s electronic medical record are preferred.
Manual anesthesia charts should allow for the registration of HR, BP, SpO₂, EtCO₂, and processed EEG (if necessary) no less frequently than every 5 minutes, and other parameters no less frequently than every 15 minutes.
Additional values should be recorded if significant changes occur within these intervals. In emergency situations, recordkeeping can be challenging; gaps in records should be filled as soon as the clinical situation allows, using trend data stored in monitoring devices.
FAQ
1. What is considered basic monitoring during anesthesia?
Minimum set of observations and devices for controlling oxygenation, ventilation, circulation, and temperature: SpO₂, ECG, blood pressure (BP)/heart rate (HR), ventilation assessment, and capnography for general anesthesia, oxygen supply control, and temperature monitoring as indicated.
2. Why is pulse oximetry mandatory for all patients?
SpO₂ is the fastest way to detect hypoxemia; with proper alarms, it allows for the detection of problems before clinical signs of cyanosis appear.
3. Why is capnography necessary if SpO₂ is normal?
SpO₂ may remain normal with supplemental oxygen even in the case of hypoventilation or apnea, whereas capnography immediately detects ventilation disturbances, obstructions, and circuit disconnections.
4. How often should blood pressure be measured during general anesthesia?
In most standards, BP is measured with non-invasive method (NIBP) and documented regularly, typically at intervals of no less than 5 minutes, unless indications call for more frequent monitoring or invasive BP measurement.
5. Which monitor alarm parameters are most important?
Those that alert to threats to oxygenation and ventilation: SpO₂, EtCO2, apnea, high airway pressure, critical BP, and HR limits.
6. Do all patients require neuromuscular blockade monitoring (TOF)?
It is not mandatory for all patients but is extremely important when using neuromuscular blocking agents (NMBAs) to avoid residual muscle relaxation and enhance extubation safety.
7. When is temperature monitoring essential?
For prolonged surgeries, in children and the elderly, during major abdominal/orthopedic interventions, significant body exposure, and during active warming — to prevent overheating.
8. Which aspects are often overlooked in basic monitoring?
Continuity of observation during the stages of induction and awakening, monitoring in the recovery room and intensive care unit/during transportation, proper setting of alarms, and clinical interpretation of data, not mere “observation of numbers.”
References
1.
VOKA 3D Anatomy & Pathology – Complete Anatomy and Pathology 3D Atlas [Internet]. VOKA 3D Anatomy & Pathology.
Available from: https://catalog.voka.io/
2.
Klein, A.A., Meek, T., Allcock E. (2021). Recommendations for standards of monitoring during anaesthesia and recovery 2021: Guideline from the Association of Anaesthetists. Anaesthesia. 76(9):1212-1223. doi: 10.1111/anae.15501.
3.
Wollner, E., Nourian, M. M., Booth W. (2020). Impact of capnography on patient safety in high- and low-income settings: a scoping review. British Journal of Anaesthesia. 125 (1): 88-103. 10.1016/j.bja.2020.04.057.
4.
Iohom, G. Basic patient monitoring during anesthesia [Internet]. In: Post TW, editor. UpToDate [Internet]. Waltham (MA): UpToDate; 2026 [updated 2025 Oct 2; cited 2026 Feb].